An acutely developing, life-threatening pathological process caused by the action of a superstrong irritant on the body and characterized by severe disturbances in the activity of the central nervous system, blood circulation, respiration and metabolism (for example, pain shock).
General ideas about shock, types of shock and methods of treating shock conditions
Shock is defined as a state of extreme reduction in blood pressure, accompanied by a decrease in oxygen supply to the tissues and the accumulation of metabolic end products. Depending on the cause that caused it, the first aid tactics will also differ, however, in any case, the resuscitation algorithm will require quick, accurate actions. What types of shock exist and what can be done for the victim before the arrival of an ambulance - MedAboutMe will tell you about this.
Shock is understood as a pathological condition that is the result of decompensation of the body's defense systems in response to a powerful irritating factor. In fact, the human body can no longer cope with the pathological process on its own (whether it be intense pain or an allergic reaction), and a decompensation reaction develops that affects the nervous, cardiovascular, and hormonal systems. It is believed that for the first time such a condition was described by the great ancient physician Hippocrates, but the term “Shock” itself was proposed only in the 18th century. Since that time, an active scientific study of the state of shock begins, theories are proposed to explain the development and effect of shock, methods of treating shock are being developed.
At the moment, shock is considered as part of the adaptation syndrome, which includes 3 stages:
Compensation.
After exposure to an aggressive irritating factor, the body retains the ability to cope with changing conditions. Perfusion (blood flow) in vital organs (brain, heart, kidneys) is maintained in sufficient volume. This stage is completely reversible.
- Decompensation.
After exposure to an aggressive irritating factor, the body already loses the ability to cope with changing conditions. Perfusion (blood flow) in vital organs progressively decreases. This stage without timely intensive treatment is irreversible.
Terminal stage.
At this stage, even intensive therapy is not able to restore the activity of vital organs. The development of the terminal stage leads to the death of the organism.
Symptoms of shock include:
- Lowering blood pressure
- Cardiopalmus
- Reduced urine output (up to its complete absence)
- Violation of the level of consciousness (characterized by a change in the period of excitation by a period of inhibition)
- Centralization of blood circulation (decrease in temperature, pallor of the skin, weakness)
Types of shock

There are several classifications of the state of shock, depending on the factors that cause it, such as hemodynamic disorders, and clinical manifestations.
In more detail we will consider all types of shock in the paragraphs specially designated for this, here we will try to give a general classification.
Classification by type of hemodynamic disorder
Lowering blood pressure by reducing the volume of circulating blood. The cause may be: blood loss, burns, dehydration.
The heart is unable to adequately contract and maintain sufficient levels of pressure and perfusion. The cause may be: heart failure, myocardial infarction, arrhythmias.
- distributional shock.
Reduction of pressure due to the expansion of the vascular bed with a constant volume of circulating blood. The cause may be: toxic poisoning, anaphylaxis, sepsis.
- obstructive shock.
The cause may be: Pulmonary embolism, tension pneumothorax.
- dissociative shock.
Acute hypoxia due to a violation of the structure of hemoglobin. Could be due to carbon monoxide poisoning
Classification by pathogenesis
- Neurogenic shock (damage to the nervous system leading to dilation of the vascular bed, usually a spinal injury)
- Anaphylactic shock (acute progressive allergic reaction)
- Septic shock
- Infectious-toxic shock
- Combined shock (a complex reaction that includes various pathogenesis of a shock state)
Clinical classification
- Compensated.
The patient is conscious, the pulse is slightly increased (~100 beats per minute), the pressure is slightly reduced (systolic at least 90 mm Hg), weakness, slight lethargy.
- Subcompensated.
The patient is conscious, stunned, lethargic, weakness grows, the skin is pale. The heart rate increases (up to 130 per minute), the pressure drops (systolic at least 80 mm Hg), the pulse is weak. Correction of the condition requires medical intervention, intensive care.
- Decompensated.
The patient is lethargic, consciousness is disturbed, the skin is pale. Pulse weak filling "threaded" more than 140 beats per minute, arterial pressure is steadily reduced (systolic less than 70 mm Hg). Violation of urine output (up to complete absence). The prognosis without adequate therapy is unfavorable.
- Irreversible.
The patient's level of consciousness is . The pulse on the peripheral arteries is not detected, blood pressure may also not be detected or is at a very low level (systolic less than 40 mm Hg). Lack of urine output. Reflexes and reactions to pain are not traced. Breathing is barely perceptible, irregular. The prognosis for life in such a situation is extremely unfavorable, intensive therapy does not lead to a positive effect.

One of the most formidable complications of allergic reactions is anaphylactic shock. It proceeds as immediate hypersensitivity and is a life-threatening condition. The rate of development of anaphylactic shock is quite high and ranges from several seconds to several hours after the reaction with the allergen. Any substance can act as an allergen, but most often these are drugs, food, chemicals, poisons. At the initial meeting of the body with the allergen, anaphylactic shock does not develop, however, the sensitivity to this allergen sharply increases in the body. And already with the repeated meeting of the body with the allergen, the development of anaphylactic shock is possible.
Clinical symptoms of anaphylactic shock are as follows:
- Pronounced local reaction, accompanied by extensive swelling, pain, fever, redness, rash
- Itching, which may become generalized
- Drop in blood pressure and increased heart rate
- Quite often, extensive swelling of the airways occurs, which can lead to the death of the patient.
For anaphylactic shock, first aid includes:
- call an ambulance
- Giving the patient a horizontal position with raised legs
- Ensure the flow of fresh air into the room, unfasten clothes, free the oral cavity from foreign objects (chewing gum, dentures)
- If anaphylactic shock has developed in response to an insect bite or an injection of a drug, then ice should be applied to the bite site, and a tourniquet should be applied above the bite.
The ambulance team has medications for the treatment of anaphylactic shock and can urgently hospitalize the patient in a hospital.
At the stage of medical care, adrenaline is injected, which quickly constricts blood vessels and expands the bronchi, increases blood pressure. Prednisolone is also introduced, which contributes to the active regression of the allergic reaction. Antihistamines (diphenhydramine, tavegil) are antagonists of histamine, which underlies the allergic reaction. An isotonic solution is injected intravenously. oxygen inhalation. Symptomatic therapy is carried out. In some cases, tracheal intubation is required, with severe laryngeal edema, a tracheostomy is applied.
As a preventive measure for anaphylactic shock, those drug or food allergens that can provoke a shock state should be avoided. It is desirable to have an emergency first aid kit in the house, including adrenaline, prednisolone or dexamethasone, isotonic solution, diphenhydramine, aminophylline, syringes and droppers, alcohol, bandage and tourniquet.
Infectious-toxic shock
The rapid drop in blood pressure in response to toxins released by bacteria is called toxic shock. The risk group includes diseases caused by coccal microorganisms: pneumonia, tonsillitis, sepsis, etc. Especially often, infectious-toxic shock develops against the background of reduced immunity in HIV infection, diabetes mellitus.
The main symptoms of infectious-toxic shock:
- Fever (above 390C)
- Decreased blood pressure (systolic below 90 mmHg)
- Impaired consciousness (depending on severity of shock)
- Multiple organ failure
Treatment for toxic shock includes:
- Treatment is carried out in the intensive care unit
- Prescribing antibiotics (cephalosporins, aminoglycosides)
- Corticosteroid drugs (prednisolone, dexamethasone)
- Massive infusion therapy
- Heparin (prevention of thrombosis)
- Symptomatic therapy
Infectious-toxic shock is a serious disease with a high mortality rate that requires immediate medical attention. Also, with this type of shock, there is a risk of developing the following complications:
- DIC syndrome (impaired coagulation system)
- Multiple organ failure (renal, pulmonary, cardiac, hepatic)
- Relapse of toxic shock
The prognosis of the disease is relatively favorable, subject to timely complex treatment.

Under cardiogenic shock understand the state of dysfunction of the pumping function of the left ventricle of the heart, leading to a persistent decrease in blood pressure, hypoxia and impaired microcirculation in organs and tissues. The causes of cardiogenic shock are: arrhythmias, severe injuries of the heart muscle, leading to a violation of its integrity, acute myocardial infarction.
There are several subtypes of cardiogenic shock:
- True
- Reflex
- Arrhythmogenic
Cardiogenic shock symptoms:
- Persistent hypotension against the background of heart pathology (systolic pressure is maintained at a level of less than 90 mm Hg)
- Tachycardia or bradycardia (depending on severity of shock)
- Centralization of blood circulation (pale and cool to the touch skin)
- Decreased urine output
- Impairment of consciousness (up to complete loss)
The severity of the manifestation of certain symptoms of cardiogenic shock on the part of the patient is affected by: age, the presence of concomitant pathologies, the duration of shock, the nature and extent of damage to the heart muscle, and the timeliness of medical care.
True cardiogenic shock
The cause of this condition is the death of at least 40% of the cardiomyocytes of the left ventricle of the heart. The prognosis for this type of shock is poor. The remaining capable cardiomyocytes are not able to provide adequate contractile activity of the heart, leading to distinct severe clinical manifestations of cardiogenic shock. Compensatory mechanisms for maintaining blood pressure (through the renin-angiotensin-aldosterone, corticoid, sympathetic-adrenal systems) are not able to fully compensate for hypotension. There is a spasm of the vascular bed and hypercoagulability, leading to DIC.
reflex shock
Reflex cardiogenic shock develops as a response of the heart to pain caused by myocardial infarction (especially infarction of the posterior wall of the heart). The reason for the development of pathology is precisely the reflex mechanism, and not the amount of damage to the heart muscle. As a reflex to pain, there is a violation of vascular tone, a decrease in blood flow to the left ventricle of the heart and, as a result, a decrease in the volume of blood ejected by the heart. With this type of shock, the prognosis is favorable, it is stopped by the appointment of analgesics and infusion therapy.
Arrhythmogenic shock
Arrhythmogenic shock is formed due to arrhythmias and blockades of the conduction pathways of the heart. The prognosis is favorable, the state of shock is stopped with timely treatment of cardiac arrhythmias. The following can lead to arrhythmogenic shock: ventricular tachycardia, AV blockade of 2-3 degrees.

Hypovolemic shock develops as a result of a sharp decrease in circulating blood volume. The reasons for this condition may be:
- Blood loss as a result of injury to the main vessels, extensive fractures, during surgical interventions, etc.
- Indomitable vomiting in violation of water and electrolyte balance
- Profuse diarrhea in some infectious diseases
- extensive burns
- Intestinal obstruction
The degree of clinical manifestations of hypovolemic shock directly depends on the amount of fluid lost (or the volume of circulating blood):
- The loss does not exceed 15%.
As such, there are no shock symptoms, but there may be slight thirst and some increase in heart rate of 10-20 beats per minute compared to the individual norm. The condition is compensated by the internal reserves of the body
- The loss does not exceed 25%.
The feeling of thirst increases, blood pressure decreases and the pulse rate increases. In an upright position, dizziness is felt.
- The loss does not exceed 40%.
Persistent hypotension (systolic pressure 90 mmHg and below), pulse rate exceeds 110 beats per minute. There is marked weakness, pallor of the skin, decreased urine output.
- The loss exceeds 40%.
Violation of the level of consciousness, severe pallor of the skin, the pulse on the periphery may not be felt, persistent hypotension, lack of urine. This condition can threaten the health and life of the patient, intensive correction of hypovolemia is necessary.
Treatment of hypovolemic shock directly proceeds from the cause of its cause. If this is bleeding, then the bleeding must be stopped, if the infectious process is antibiotic therapy, intestinal obstruction is resolved by surgery. In addition, at all stages of treatment, it is necessary to carry out massive infusion therapy in order to correct the water and electrolyte balance. For this purpose, a central venous access is performed (for example, the subclavian vein is catheterized). Transfusion of donated blood and plasma has proven itself as a treatment for hypovolemic shock, especially in the case of a decrease in hemoglobin and protein levels. With timely relief of the cause of hypovolemic shock and normalization of the water and electrolyte balance, the prognosis for the patient is favorable.
Other causes of shock
As mentioned above, shock can also be caused by carbon monoxide poisoning. The thing is that carbon monoxide has the ability to integrate into the hemoglobin molecule and impede the transport of oxygen to organs and tissues. Carbon monoxide is formed as a result of combustion with limited access to oxygen. This situation occurs during fires in enclosed spaces. Clinical manifestations directly depend on the concentration of carbon monoxide in the air and the duration of its inhalation. The main symptoms are as follows:
- Dizziness, weakness
- Disturbance of consciousness
- Increased blood pressure and pulse rate
- Nausea, vomiting
- Redness of the skin and mucous membranes
- convulsive syndrome
Despite the fact that blood pressure rises, hypoxia increases in the body due to a violation of oxygen transport to the tissues. Carbon monoxide poisoning is the leading cause of death in fires. It should be remembered that the filtering gas mask for protection against carbon monoxide must be equipped with a hypocalite cartridge.
To prevent the development of shock caused by carbon monoxide poisoning, the victim must:
- remove from carbon monoxide
- provide access to fresh air, wear an oxygen mask
- there is a special antidote for carbon monoxide "Acyzol". This drug can also be used as a means of preventing carbon monoxide poisoning.
With a mild degree of poisoning, these measures are quite enough, but in any case it is advisable to consult a doctor. Additional methods of treatment and prevention include hyperbaric oxygen therapy, ultraviolet irradiation, symptomatic therapy. To prevent the development of inflammatory diseases of the upper respiratory tract, it is advisable to prescribe antibiotics.

The effect of shock on the internal organs occurs due to a number of factors. These include lowering blood pressure, insufficient blood supply, perfusion, organs and tissues, hypoxia, edema, acid-base and water-electrolyte imbalance.
Each type of shock state has its own individual mechanisms of pathogenesis, however, in general, any shock leads to the development of hypoxia against the background of inadequate microcirculation, which is the cause of multiple organ failure. The effect of shock is the more dangerous, the less resistant the organ to hypoxia.
So, for example, the brain is most sensitive to oxygen deficiency and suffers first when a shock occurs. This is manifested by dizziness, headache, drowsiness, lethargy. Shock symptoms progress according to the severity of the patient's condition and may be accompanied by loss of consciousness and inhibition of reflex activity.
The effect of shock on the internal organs is not only physiological, but also morphological. So, if the cause of death of the patient was shock, then this condition will directly affect the internal organs. There is even a special concept of "shock organ", which characterizes the morphological changes that have arisen in a particular organ.
- "Shock Kidney"
Against the background of shock, urine output decreases, up to its complete absence, protein and red blood cells can be observed in the urine. In the blood, the content of urea and creatinine increases. On section, the cortical layer of such a kidney looks pale and edematous. The pyramids are brown. Under the microscope, anemia of the cortical zone, necrosis of the epithelium of the convoluted tubules, edema of the interstitium are visible.
- "Shock Liver"
This condition is often accompanied by the development of a shock kidney as part of the syndrome of multiple organ failure and develops, as a rule, in the phase of shock decompensation. Liver enzymes increase in the blood. On the section, the liver has a pale, yellowish tint. Hepatocytes lack glycogen. Due to hypoxia, necrosis occurs in the central part of the hepatic lobules.
- "Shock Lung"
In the clinical literature, this condition is also referred to as Adult Respiratory Distress Syndrome. The lung is unevenly filled with blood, edema of the interstitium develops, multiple necrosis of the lung tissue, hemorrhages are formed. With the development of a shock lung, pneumonia always joins.
- "Shock Heart"
The phenomena of hypoxia are also clearly expressed in the heart. The muscle cells of the heart are deprived of glycogen, they develop the phenomena of dystrophy, the accumulation of lipids, and foci of necrosis are formed.
- "Shock Gut"
Multiple hemorrhages are observed in the intestine, ulceration areas are formed in the mucous layer. The loss of the barrier function of the intestinal wall leads to the release of bacteria and their toxins, which aggravates the severity of the condition of such a patient.
It should be remembered that the morphological changes in the organs described above during shock develop into the decompensation phase and into the terminal phase. They are not purely specific, but only complement the overall picture of the effect of shock on internal organs.
Painful shock
Quite often you can hear or read such a term as "Pain shock". Above, we have analyzed the main types of shock, according to the main classifications used in medical practice, and pain shock is not mentioned among them, what's the matter? The answer is that the pain itself does not cause shock. Yes, pain in some situations is quite strong, sometimes painful, sometimes with loss of consciousness, but it is not the cause of shock. In case of trauma, especially with extensive trauma, pain always accompanies the state of shock, supplementing the general clinical symptoms. The term "pain shock" is most often used as a synonym for traumatic shock, and traumatic shock is a special case of hypovolemic shock, which is based on the loss of circulating blood volume by the body. In principle, it is not forbidden to call a traumatic shock pain, but such non-professional terminology is unacceptable in a medical conversation.

Traumatic shock develops as a result of external excessive effects on the body (trauma of any origin, extensive burns, electric shock). Two types of factors play a role in the development of traumatic shock:
- The nature of the injury (fracture, burn, blunt trauma, incised wound, electrical injury, etc.)
- Concomitant conditions (age of the patient, duration of hypotension, stress, hunger, ambient temperature, etc.)
In the development of the clinical picture of traumatic shock, there are 2 main phases, which were the first to be described in detail in his works by the outstanding surgeon N.I. Pirogov:
- arousal (erectile)
- braking (torpid)
During the erectile phase, there is a general activation of the patient, his endocrine and sympathetic systems. The patient is conscious, reflexes are brisk, he is excessively restless, the pupils are somewhat dilated, the skin is pale, the pulse is quickened, the blood pressure is increased. Most often, the erectile phase of shock accompanies trauma to the central nervous system. This phase is observed in 1/10 of all clinical cases of traumatic shock.
During the torpid phase, a general lethargy of the patient is observed, with a gradual regression of activity, both in terms of his motor activity and emotionally. The patient's consciousness is disturbed, he is lethargic, adynamic, the skin is pale, cold to the touch, hypotension, the pulse is rapid, superficial, urine output is reduced. This phase is observed in 9/10 of all clinical cases of traumatic shock.
According to the clinical picture, traumatic shock is divided into 3 degrees:
- A mild degree of shock develops, as a rule, with an isolated injury, the volume of blood loss is small and amounts to 20% of the volume of circulating blood. A person in mild shock remains conscious, the pressure is slightly reduced, the pulse is quickened, weakness is subjectively felt. The prognosis in this case is favorable, anti-shock measures are symptomatic.
- The average degree of shock develops, as a rule, with severe isolated or combined trauma. The volume of blood loss is approximately 20 to 40% of the volume of circulating blood. A person in shock is stunned, the skin is pale, hypotension reaches a level below 90 mm Hg, the pulse is accelerated to 110 beats per minute. The prognosis in this case is closely related to the accompanying conditions that exacerbate the course of the shock. If medical care is provided in a timely manner, then the prognosis for further recovery is favorable.
- A severe degree of shock develops, as a rule, with extensive concomitant trauma with injury to the main vessels and vital organs. A person in severe shock is adynamic, consciousness is disturbed, skin is pale, reflexes are inhibited, Arterial systolic pressure can drop below 60 mm Hg, pulse is frequent, weak, may not be heard on peripheral arteries, breathing is rapid, superficial, urine is not excreted . The volume of blood loss exceeds 40% of the volume of circulating blood. The prognosis in this case is not favorable.
Treatment of traumatic shock involves early diagnosis and an integrated approach. Therapeutic measures should be aimed at eliminating the factors that cause shock, factors that aggravate the course of shock and maintain body homeostasis. The first thing that needs to be stopped in case of injury is pain. To achieve this rule, the following actions are rendered:
- Careful transportation of the patient from the lesion
- Immobilization of the damaged area of the body
- Anesthesia (narcotic and non-narcotic analgesics, novocaine blockades, anesthesia)
After anesthesia, the source of bleeding is identified and eliminated. can be both external and internal. Stopping bleeding is temporary (application of a pressure bandage, tourniquet) and final (ligation of the vessel or its reconstruction). Accumulations of blood in body cavities (abdominal, pleural) are subject to evacuation by drainage. Simultaneously with stopping bleeding, it is necessary to provide infusion correction of the lost volume of fluid. For this, colloidal, crystalloid solutions, plasma and blood components are used. With a persistent decrease in blood pressure, the following drugs with pressor properties are used: norepinephrine, dopmin, mezaton. Corticosteroids (solumedrol, dexamethasone) are also administered.
Counteracting respiratory failure is also an integral component in the treatment of traumatic shock. It is necessary to restore airway patency, establish adequate ventilation, eliminate pneumothorax, hemothorax, provide inhalation with oxygen, and if spontaneous breathing is impossible, transfer the patient to artificial ventilation (ventilator). Correction of homeostasis is carried out by normalizing the water-electrolyte balance and pH balance.
The main point of the final treatment of traumatic shock is the implementation of surgical intervention. Depending on the type of injury, the operation helps to stop bleeding, asphyxia, restore the integrity of damaged organs and tissues, remove accumulated blood, etc. All of the above measures to combat traumatic shock are, in fact, preoperative preparation of the patient in order to recover from the state of shock. During the operation, it is necessary to monitor vital signs, compensate for blood loss and hypoxia. In a state of shock, it is permissible to perform operations only for health reasons (tracheostomy in case of asphyxia, stopping ongoing bleeding, eliminating tension pneumothorax).
How to quickly assess that a person is in shock
The clinical symptoms of shock are quite characteristic. It includes a violation of the level of consciousness, a persistent decrease in blood pressure, an increase in heart rate and pulse. Later, with the progression of shock, multiple organ failure increases due to impaired perfusion and hypoxia in organs and tissues.
Any shock is preceded by a cause that causes it. So with anaphylactic shock there is always an allergen substance, with cardiogenic shock - a violation of the heart, etc.
In traumatic shock, it is possible to assess the patient's condition by the nature of the injury.
- Mild degree of shock: extensive soft tissue injury, fracture of the shoulder, lower leg, closed fracture of the femur, detachment of the foot or hand, acute blood loss (up to 1.5 liters).
- Medium degree of shock: a combination of two signs of a mild degree of shock, a pelvic fracture, acute blood loss (up to 2 liters), a shin or forearm tear, an open hip fracture, a penetrating wound to the chest or abdomen.
- Severe shock: a combination of two signs of an average degree of shock or three signs of a mild degree of shock, acute blood loss (over 2 liters), hip avulsion.
For a preliminary assessment of the severity of traumatic shock, the so-called "shock index" is used. The shock index is calculated by dividing the heart rate (beats per minute) by the systolic blood pressure (in mm Hg). Under normal conditions, the index is 0.5, with mild shock it ranges from 0.6 to 0.8, with average shock it is from 0.9 to 1.2, and with severe shock it exceeds 1.3.

If suddenly such a situation happened that a person in a state of shock was next to you, do not pass by. Another important rule is not to panic. Calm down, assess the situation, think about how you can help. It should be remembered that a person in a state of shock cannot help himself. Therefore, call an ambulance and, preferably, stay nearby until the doctors arrive. In principle, this is all that is required of you at this stage. You can also try to find out the cause and circumstances of the shock, to eliminate the damaging factor, if possible. In some cases, it is possible to stop external bleeding with improvised means. You should not rush to the victim and give him cardiopulmonary resuscitation if you do not know how to do this in practice.
shock treatment
Sometimes you can find such headings as "shock treatment". Yes, this type of treatment does exist, only it is called completely “electroshock therapy”. Treatment is carried out due to electric current, and not a shock state. The state of shock itself cannot cure any pathology, since shock itself is a serious pathological condition that requires medical intervention.
The confusion of terms, of course, is present and, in order to understand, we will briefly describe here electroconvulsive therapy (synonyms: electroconvulsive or electroconvulsive therapy). This type of treatment is based on the effect of electric current on the human brain. Electroshock therapy is used in psychiatric practice for the treatment of schizophrenia and severe depressive disorders. This method has a narrow list of indications for use and a number of side effects.
First aid for shock
As noted above, shock comes down to a small list of rules that are not difficult to remember. Of course, one should take into account the reason that caused the shock, but the general rules are quite similar. Next, an approximate algorithm of actions will be described when a person in shock is detected. In principle, the most important thing is not to remain indifferent and call an ambulance in a timely manner. It is also important not to panic, especially to yell at a patient who is in a state of shock. Hitting him on the cheeks and bringing him to his senses is also not recommended, external aggression can only aggravate the already grave condition of the victim. After calling an ambulance, stay close to the victim. All other measures indicated below in the algorithm are, of course, important, but are of a secondary nature, and no one forces you to perform them.
Do not perform cardiopulmonary resuscitation if you do not have experience with it. Firstly, the reason that caused the state of shock in a person is not always immediately reliably known, especially if it is a stranger on the street. Second, inept performance of cardiopulmonary resuscitation can exacerbate the severity of a person in shock.
The same situation is with the application of a tourniquet. It is necessary to remember the basic rules for its imposition:
- A tourniquet is applied to the limb above the level of bleeding
- The tourniquet must not be applied to a naked body, place a piece of clothing under it
- The tourniquet is tightened to stop arterial bleeding
- It is necessary to indicate the exact time of applying the tourniquet
- The tourniquet should be clearly visible, warn the ambulance doctor about this

Emergency care for shock includes:
- Anesthesia. This is especially true in traumatic shock. Narcotic and non-narcotic analgesics are used, sometimes anesthesia is required.
- In anaphylactic shock, the administration of adrenaline and antihistamines and glucocorticoids is necessary.
- In case of infectious toxic shock, it is necessary to select adequate antibiotic therapy.
- Hypovolemic shock requires massive fluid therapy and elimination of the source of hypovolemia (especially if it is ongoing bleeding).
- If cardiogenic shock is caused by an arrhythmia, then antiarrhythmic drugs are prescribed.
- In cases of combined shock, treatment begins with the elimination of life-threatening conditions.
Operational benefits are produced after stabilization of the patient's hemodynamics. An exception can only be operations for vital indications (continued bleeding, tracheostomy in case of asphyxia).
Help with shock: an algorithm of actions
An approximate algorithm of action in case of shock is as follows:
- Call an ambulance. Self-medication with developed shock is contraindicated.
- Do not leave a person in shock alone, monitor his condition.
- If possible, the damaging factor should be eliminated. For example, stop the administration of the drug if it caused anaphylaxis, apply a bandage or tourniquet for external bleeding.
- If a person in shock is unconscious, then his head must be turned to the side. This measure prevents asphyxia.
- Unfasten tight clothing, ensure the flow of fresh air into the room, free the patient's mouth from foreign objects (chewing gum, dentures).
- It is necessary to prevent hypothermia of the patient, cover him with a blanket or jacket.
- In case of injury, fracture, the damaged part of the body must be immobilized.
- Transportation of a person in shock should be carried out carefully, without sudden movements.
- After the arrival of the ambulance, give the information you have about the person in shock. Indicate the exact time of applying the tourniquet, if one was applied.

When anaphylactic shock develops, first aid is as follows:
- It is necessary to immediately stop the contact of the allergen substance with the patient: no longer inject the drug that caused anaphylaxis, apply a tourniquet above the insect bite, apply ice to the wound.
- Call an ambulance
- Lay the patient down, slightly raise the legs
- Free the oral cavity from foreign objects (chewing gum, dentures)
- Provide oxygen access to the room, unfasten tight clothing
- Take an antihistamine
- Stay close to the patient until the ambulance arrives
The ambulance team has medications for the treatment of anaphylactic shock, therapeutic measures will be as follows:
- The introduction of adrenaline. This drug quickly raises blood pressure, reduces swelling, dilates the bronchi
- Introduction of glucocorticoids. The drugs of this group have an antiallergic effect, increase blood pressure
- Administration of antihistamines.
- Euphyllin contributes to the regression of the resulting bronchospasm
- Oxygen inhalation reduces the effects of hypoxia
- Drugs can be administered repeatedly to achieve a therapeutic effect
In contact with
classmates
General information
This is a severe condition where the cardiovascular system cannot keep up with the body's blood supply, usually due to low blood pressure and damage to cells or tissues.
Causes of shock
Shock can be caused by a condition in the body where blood circulation is dangerously low, such as heart disease (heart attack or heart failure), large blood loss (hemorrhage), dehydration, severe allergic reactions, or blood poisoning (sepsis).
Shock classification includes:
- cardiogenic shock (associated with cardiovascular problems),
- hypovolemic shock (caused by low blood volume),
- anaphylactic shock (caused by allergic reactions),
- septic shock (caused by infections)
- neurogenic shock (disorders of the nervous system).
Shock is a life-threatening condition and requires immediate medical treatment, and emergency care is not ruled out. The patient's condition in shock can deteriorate rapidly, be prepared for primary resuscitation.
Shock Symptoms
Symptoms of shock may include fear or excitement, blue lips and nails, chest pain, confusion, cold, wet skin, reduced or stopped urination, dizziness, fainting, low blood pressure, paleness, excessive sweating, rapid heart rate, shallow breathing, unconsciousness , weakness.
First aid for shock
Check the victim's airway and give artificial respiration if necessary.
If the patient is conscious and has no injuries to the head, limbs, back, lay him on his back, while the legs should be raised by 30 cm; keep your head down. If the patient has received an injury in which the raised legs cause a feeling of pain, then do not raise them. If the patient has received a severe injury to the spine, leave him in the position in which he was found, without turning over, and provide first aid by treating wounds and cuts (if any).
The person should remain warm, loosen tight clothing, do not give the patient any food or drink. If the patient is vomiting or drooling, turn his head to the side to ensure the outflow of vomit (only if there is no suspicion of a spinal cord injury). If, nevertheless, there is a suspicion of damage to the spine and the patient is vomiting, it is necessary to turn it over, fixing the neck and back.
Call an ambulance and continue to monitor vital signs (temperature, pulse, respiratory rate, blood pressure) until help arrives.
Preventive measures
Shock is easier to prevent than to treat. Prompt and timely treatment of the underlying cause will reduce the risk of severe shock. First aid will help control the state of shock.
Shock is a pathological change in the functions of the vital systems of the body, in which there is a violation of breathing and blood circulation. This condition was first described by Hippocrates, but the medical term appeared only in the middle of the 18th century. Since various diseases can lead to the development of shock, for a long time scientists have proposed a large number of theories of its occurrence. However, none of them explained all the mechanisms. It has now been established that shock is based on arterial hypotension, which occurs with a decrease in circulating blood volume, a decrease in cardiac output and total peripheral vascular resistance, or with a redistribution of fluid in the body.
Manifestations of shock
The symptoms of shock are largely determined by the cause that led to its appearance, but there are common features of this pathological condition:
- violation of consciousness, which can be manifested by excitement or depression;
- decrease in blood pressure from insignificant to critical;
- an increase in heart rate, which is a manifestation of a compensatory reaction;
- centralization of blood circulation, in which there is a spasm of peripheral vessels, with the exception of the renal, cerebral and coronary;
- pallor, marbling and cyanosis of the skin;
- rapid shallow breathing that occurs with an increase in metabolic acidosis;
- change in body temperature, usually it is low, but during the infectious process it is increased;
- pupils are usually dilated, reaction to light is slow;
- in especially severe situations, generalized convulsions, involuntary urination and defecation develop.
There are also specific manifestations of shock. For example, when exposed to an allergen, bronchospasm develops and the patient begins to choke, with blood loss, a person experiences a pronounced feeling of thirst, and with myocardial infarction, chest pain.
Degrees of shock
Depending on the severity of shock, four degrees of its manifestations are distinguished:
- Compensated. At the same time, the patient's condition is relatively satisfactory, the function of the systems is preserved. He is conscious, systolic blood pressure is reduced, but exceeds 90 mm Hg, pulse is about 100 per minute.
- Subcompensated. Violation is noted. The patient's reactions are inhibited, he is lethargic. The skin is pale, moist. The heart rate reaches 140-150 per minute, shallow breathing. The condition requires prompt medical attention.
- Decompensated. The level of consciousness is reduced, the patient is severely retarded and reacts poorly to external stimuli, does not answer questions or answers in one word. In addition to pallor, marbling of the skin is observed due to impaired microcirculation, as well as cyanosis of the fingertips and lips. The pulse can be determined only on the central vessels (carotid, femoral artery), it exceeds 150 per minute. Systolic blood pressure is often below 60 mmHg. There is a violation of the internal organs (kidneys, intestines).
- Terminal (irreversible). The patient is usually unconscious, breathing is shallow, the pulse is not palpable. The usual method with the help of a tonometer often does not determine the pressure, the heart sounds are muffled. But blue spots appear on the skin in places where venous blood accumulates, similar to cadaveric ones. Reflexes, including pain, are absent, the eyes are motionless, the pupil is dilated. The prognosis is extremely unfavorable.
The Algover shock index, which is obtained by dividing heart rate by systolic blood pressure, can be used to determine the severity of the condition. Normally, it is 0.5, with 1 degree -1, with the second -1.5.
Types of shock
Depending on the immediate cause, there are several types of shock:
- Traumatic shock resulting from external influences. In this case, there is a violation of the integrity of some tissues and the occurrence of pain.
- Hypovolemic (hemorrhagic) shock develops when the volume of circulating blood decreases due to bleeding.
- Cardiogenic shock is a complication of various heart diseases (, tamponade, aneurysm rupture), in which the ejection fraction of the left ventricle decreases sharply, as a result of which arterial hypotension develops.
- Infectious-toxic (septic) shock is characterized by a pronounced decrease in peripheral vascular resistance and an increase in the permeability of their walls. As a result, there is a redistribution of the liquid part of the blood, which accumulates in the interstitial space.
- develops as an allergic reaction in response to intravenous exposure to a substance (prick, insect bite). In this case, histamine is released into the blood and vasodilation, which is accompanied by a decrease in pressure.
There are other varieties of shock that include various symptoms. For example, burn shock develops as a result of trauma and hypovolemia due to large fluid losses through the wound surface.
Help with shock
Every person should be able to provide first aid for shock, since in most situations minutes count:
- The most important thing to do is to try to eliminate the cause that caused the pathological condition. For example, when bleeding, you need to clamp the arteries above the injury site. And with an insect bite, try to prevent the poison from spreading.
- In all cases, with the exception of cardiogenic shock, it is advisable to raise the victim's legs above the head. This will help improve the blood supply to the brain.
- In cases of extensive injuries and suspected spinal injury, it is not recommended to move the patient until the ambulance arrives.
- To make up for fluid losses, you can give the patient a drink, preferably warm, water, as it will be absorbed faster in the stomach.
- If a person has severe pain, he can take an analgesic, but it is not advisable to use sedatives, since this will change the clinical picture of the disease.
Emergency physicians in cases of shock use either solutions for intravenous infusions or vasoconstrictor drugs (dopamine, adrenaline). The choice depends on the specific situation and is determined by a combination of various factors. Medical and surgical treatment of shock depends on its type. So, in case of hemorrhagic shock, it is urgent to replenish the volume of circulating blood, and in case of anaphylactic shock, antihistamine and vasoconstrictor drugs should be administered. The victim must be urgently delivered to a specialized hospital, where treatment will be carried out under the control of vital signs.
The prognosis for shock depends on its type and degree, as well as the timeliness of assistance. With mild manifestations and adequate therapy, recovery almost always occurs, while with decompensated shock, the likelihood of death is high, despite the efforts of doctors.
Did you see an error? Select and press Ctrl+Enter.
Shock is a complex phenomenon that occurs as a reaction to severe damage or injury, which is related to almost all internal organs and body systems. The circulatory organs are mainly affected.
The main signs of a state of shock are:
Sharp pain;
Blood intoxication, accompanied by an increase in body temperature;
Opening bleeding;
Cooling the body.
One of the reasons for the state of shock is toxicosis due to prolonged squeezing or trauma to soft tissues. Renal failure develops due to damage to the epithelial layer of the kidneys and blockage of the passage of the renal tubules. About the power of the shock state in case of kidney damage, conclusions can be drawn on the basis of a small amount of urine or its complete absence, even if blood pressure is normal.
A state of shock after a severe burn is characterized by a significant decrease in the mass of circulating blood due to the fact that blood plasma comes out through the broken skin.
The first stage of the state of shock is characterized by the extreme degree of excitation of the victim, his inability to understand the severity of the condition and the injuries received. At the next stage of development of the state of shock, the reaction of the victim is inhibited, the person becomes apathetic. Consciousness throughout all stages of the shock state is preserved. The skin and mucous membranes become pale.
In the state of shock of the first stage, blood pressure and heart rate do not change.
In the state of shock of the second stage, blood pressure drops significantly, the heart begins to beat more often, the pallor of the skin and visible mucous membranes increases, and the peripheral circulatory system is less active.
In the state of shock of the third stage, an extremely serious condition is observed. Arterial pressure is greatly underestimated, the heart beats very often, the pulse is characterized by weak filling. At this stage of the state of shock, there is a strong pallor of the skin, cold perspiration. With the further development of the state of shock, consciousness begins to leave the victim. Spots begin to appear on pale skin. The pulse can only be set on the main arteries.
In the treatment of shock, the same methods are used as in the case of shock of hemorrhagic origin. In a state of shock, it is extremely important to provide first aid to the victim before the ambulance arrives.
Firstly, it is necessary to restore the normal patency of the air passageways, that is, to normalize the position of the tongue, if it is sunk, use mouth-to-mouth breathing. After that, it is necessary to restore normal blood circulation with the help of intensive closed massage of the heart muscle, clamping of blood vessels, intravenous injections of the drug Polyglucin and sodium bicarbonate.
In addition to the above measures, it is necessary:
Apply sterile dressings to open wounds;
Fix fractures, if any;
Properly lay the victim;
In case of injury to the chest, give the victim a sitting position;
When receiving a traumatic brain injury, the victim is given a semi-sitting position;
When receiving an injury to the abdomen, the victim must be laid horizontally;
Injections of antispasmodics are performed if necessary;
If necessary, it is necessary to raise the legs of the victim to the elevation;
Fixation of bone fragments with an open fracture;
Warming actions to prevent hypothermia of the victim;
Give the victim as much to drink as possible if the stomach is not damaged and there is no vomiting;
Get the victim to the hospital as soon as possible.
Before using the drugs listed on the site, consult your doctor.
SHO K I E G O P R O Y A L E N I A
The term "shock" means a blow in translation. .
This is a critical state of the body between life and death, characterized by deep disorders and depression of all vital functions (respiration, blood circulation, metabolism, liver, kidney functions, etc.). A state of shock can occur with severe injuries, extensive burns and large blood loss. Pain, cooling of the body, hunger, thirst, shaking transportation of the victim contribute to the development and deepening of shock.
Shock is an active defense of the body against environmental aggression..
Depending on the cause that causes the development of a shock state, there are:
1. Shock due to external causes: - traumatic, resulting from mechanical trauma (wounds, bone fractures, tissue compression, etc.);
- burn associated with burn injury (thermal and chemical burns);
- cold , low temperature developing;
- electric resulting from an electrical injury.
2. Shock caused by exposure to internal causes:
- hemorrhagic resulting from acute and massive blood loss;
- To cardiogenic developing with myocardial infarction;
- With optic, which is a consequence of a general purulent infection in the body.
When a person is faced with the threat of death, his body in a state of stress releases a huge amount of adrenaline.
REMEMBER! A colossal release of adrenaline causes a sharp spasm of the precapillaries of the skin, kidneys, liver and intestines.
The vascular network of these and many other organs will be practically excluded from the blood circulation. And such vital centers as the brain, heart, and partly the lungs will receive much more blood than usual. There is a centralization of blood circulation in the hope that after overcoming the extreme situation, they will again be able to start normal life.
REMEMBER! The loss of 1.5 - 2 liters of blood is compensated only due to the spasm of the skin vessels and its exclusion from the blood circulation.
That is why in the first minutes of shock, thanks to the spasm of the precapillaries and a sharp increase peripheral resistance(PS), the body manages not only to maintain the level of blood pressure within normal limits, but also to exceed it even with heavy bleeding.
The first signs of shock development:
Sharp blanching of the skin;
Emotional and motor excitement;
Inadequate assessment of the situation and one's condition;
Absence of complaints of pain even with shockogenic injuries.
The ability to forget about pain at the moment of mortal danger is explained by the fact that a morphine-like substance is produced in the subcortical structures of the brain - endomorphinol( internal, own morphine). Its drug-like action induces a state of mild euphoria and relieves pain even in severe injuries.
On the other hand, pain activates functions endocrine glands and especially the adrenal glands. It is they who secrete the amount of adrenaline, the action of which will cause a spasm of the precapillaries, an increase in blood pressure and an increase in heart rate.
The adrenal cortex secretes and corticosteroids (their analogue is synthetic - prednisolone), which significantly accelerates the metabolism in tissues.
This allows the body to throw out the entire supply of energy in the shortest possible time and concentrate efforts as much as possible in order to get away from danger.
There are two phases of shock:
- short-term erictile(excitation period) phase occurs immediately after the injury and is characterized by motor and speech excitation, as well as complaints of pain. With full preservation of consciousness, the victim underestimates the severity of his condition. Pain sensitivity is increased, the voice is deaf, the words are jerky, the look is restless, the face is pale, the blood pressure is normal or high. An excited state quickly (within a few minutes), less often gradually, turns into an oppressed one, accompanied by a decrease in all vital functions.
- torpid phase (period of oppression: lat. torpidum - inhibition) is characterized by general weakness and a sharp drop in blood pressure. Breathing becomes frequent and superficial. The pulse is frequent, uneven, threadlike (hardly palpable). The face is pale, with an earthy tint, covered with cold clammy sweat. The victim is lethargic, does not answer questions, treats others indifferently, pupils are dilated, consciousness is preserved. In severe cases, vomiting and involuntary urination may occur.
This phase usually ends in death and is considered irreversible..
If within 30-40 minutes the victim does not receive medical assistance, then prolonged centralization of blood circulation will lead to gross violations of microcirculation in the kidneys, skin, intestines and other organs excluded from blood circulation. Thus, what played a protective role at the initial stage and gave a chance for salvation will become the cause of death in 30-40 minutes.
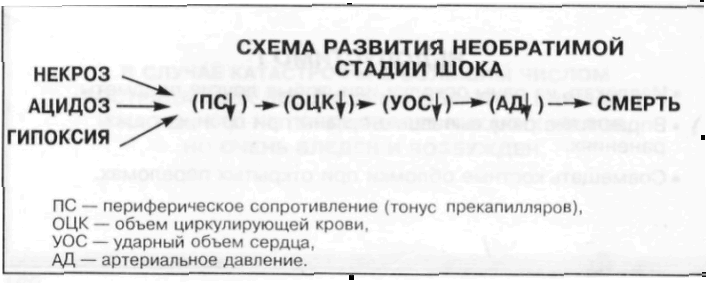
A sharp decrease in the rate of blood flow in the capillaries, up to a complete stop, will cause a violation of oxygen transport and the accumulation of incompletely oxidized metabolic products in the tissues - acidosis, lack of oxygen - hypoxia and necrosis in a living organism of individual organs and tissues - necrosis.
This stage is very quickly replaced by agony and death. .
A COMPLEX OF ANTI-SHOCK MEASURES.
It is necessary to free the victim from the action of the traumatic factor;
Ensure bleeding stops
To stabilize breathing, provide an influx of fresh air and give a position that ensures breathing;
Give painkillers (analgin, baralgin, pentalgin);
Give funds that tonic the activity of the cardiovascular system (corvalol - 10-15 drops, cordiamine, tincture of lily of the valley);
The victim should be warmed;
Give plenty of warm drink (tea, coffee, water with the addition of salt and baking soda - 1 teaspoon of salt and 0.5 teaspoon of soda per 1 liter of water);
Perform immobilization of injured body parts;
In case of cardiac arrest and breathing, urgent resuscitation measures should be taken (ventilation, external heart massage);
THE INJURED SHOULD NOT BE LEFT ALONE!
