- 1. ALGORITHMS OF RAY RESEARCH METHODS Prof. B.N. Sapranov Izhevsk State Medical Academy Course of Radiation Diagnostics and Radiation Therapy Prof.
- - Standard..." target="_blank"> 2. LEVELS OF RADIATION ALGORITHMS
- - Standard radiography
- - General purpose ultrasound
- - Linear tomography
- Television fluoroscopy
- - All Level I techniques
- - Spec. radiography techniques
- - Spec. ultrasound techniques, including dopplerography
- - Mammography
- - Osteodensitometry
- - Angiography
- - CT
- - Radionuclide methods
- - All methods of level I and II
- - MRI
- - PET
- - Immunoscintigraphy
- Informativeness..." target="_blank"> 3. Principles for choosing a visualization method
- informative
- The lowest level of exposure
- Minimum cost
- Radiologist Qualification
- Diseases..." target="_blank"> 4. Headache syndrome Main causes
- CNS diseases
- Anomalies of the QUO
- Hypertonic disease
- Vertebrobasilar insufficiency
- Level I Skull radiography
- Norm Intracranial Intracranial hypertension calcification
- Radiography of the cervical
- spine
- Level II CT, MRI CT, MRI CT
- 6. Intracranial calcifications MeduMed.Org - Medicine is Our Vocation
- 8. Lateral synostosis and spondylolysis C6-C7
- ORGANS OF THE CHEST MeduMed.Org - Honey..." target="_blank"> 9.
- ORGANS OF THE CHEST
- Acute pneumonia
- Acute pleurisy..." target="_blank"> 10.
- Acute pneumonia
- Acute pleurisy
- Spontaneous pneumothorax
- TELA
- Acute abdomen (appendicitis, cholecystitis)
- Pathology of the skeletal system
- 11. Algorithm of radiological examination in acute chest pain syndrome of non-cardiac localization NORMAL PAT. BONES? ESOPHAGUS PAT? PNEUMOTHORAX? TELA? MEDIASTINUM? PLEURISY? PRIC. IMAGE EXAMINATION GRAPHICS IMAGE ULTRASOUND Ur. II CT CT APG SKELETON SCINTIGRAPHY MeduMed.Org - Medicine - Our Vocation
- 12. Acute pleurisy
- 13. Acute pneumonia MeduMed.Org - Medicine is Our Vocation
- 14. Lung infarction MeduMed.Org - Medicine is Our Vocation
- 15. Small pneumothorax MeduMed.Org - Medicine - Our Vocation
- 16. Rib fractures in multiple myeloma
- 17. Acute pain in the chest of cardiac localization (first of all, it is necessary to exclude AMI) Main causes
- Dissecting aortic aneurysm
- TELA
- Acute pericarditis
- Acute pleurisy
- Reflux esophagitis
- Diaphragmatic hernia incarceration
- Acute abdomen (gastric ulcer perforation, cholecystitis).
- 18. Algorithm of radiological examination for acute pain in the chest of cardiac localization
- Level I ultrasound (sonography)
- 19. Coronarosclerosis MeduMed.Org - Medicine is Our Vocation
- 20. Diaphragmatic hernia MeduMed.Org - Medicine is Our Vocation
- Main reasons
- 1) coronary artery disease
- 2) Cardiomyopathy
- 3) Dry pericarditis
- 4) Stenosis of the aortic mouth
- 5) Diseases of the lungs and diaphragm
- 6) Reflux esophagitis
- 7) Axial hiatal hernia
- 8) Relaxation of the diaphragm
- 9) Intercostal neuralgia
- 22. Radiation examination algorithm for chronic pain in the heart area
- Level I Chest x-ray, ultrasound
- No changes Changes detected Lungs Heart Aortic aneurysm
- Ultrasound of the abdomen See diagrams X-ray. gr. class delayed Lv. II RDI of the esophagus, Doppler of the stomach AKG, Aortography Coronary angiography. CT with contrast.
- Level III
- MRI
- 23. Lung hypostasis MeduMed.Org - Medicine is Our Vocation
- 24. Aneurysm of the left ventricle MeduMed.Org - Medicine - Our Vocation
- 25. Aortic Aneurysm MeduMed.Org - Medicine is Our Vocation
- 26. Cardiomegaly
- 27. Aortic stenosis
- 28. Constrictive pericarditis MeduMed.Org - Medicine is Our Vocation
- 29. Relaxation of the diaphragm
- Main reasons
- 1) COPD<..." target="_blank">30. Shortness of breath
- Main reasons
- 1) COPD
- 2) Airway obstruction (intrabronchial tumors, mediastinal lymphadenopathy)
- 3) TELA
- 4) Heart disease
- 5) Diffuse interstitial focal lung diseases (toxic and allergic alveolitis, fibrosing alveolitis, pneumoconiosis, multiple metastases)
- 6) Primary pulmonary hypertension
- 7) Anemia
- 8) Obesity
- Level..." target="_blank"> 31. Imaging Algorithm for Breathlessness
- Level I CHEST RADIOGRAPHY
- 32. Emphysema
- 33. Wegener's granulomatosis
- 34. Primary pulmonary hypertension
- 35. Foreign body in the bronchus
- 36. Exogenous alveolitis
- 37. Scleroderma MeduMed.Org - Medicine is Our Vocation
- 38. Scleroderma
- 39. Pulmonary berylliosis
- 40. Sarcoidosis of the lungs MeduMed.Org - Medicine is Our Vocation
- 41. TELA MeduMed.Org - Medicine is Our Vocation
- 42. Lymphadenopathy of the mediastinum MeduMed.Org - Medicine - Our Vocation
- Main reasons
- Main reasons
- 1) Pulmonary tuberculosis
- 2) COPD (chronic bronchitis, bronchiectasis)
- 3) Central lung cancer
- 4) Compression of the trachea and main bronchi (tumorous lymphadenopathy, viral bronchoadenitis)
- 5) Lung anomalies
- Level I Chest X-ray Diagnosis is clear Diagnosis is not clear Linear tomography Functional X-ray (Sokolov's test)
- Level II CT, APG
- 45. Hematogenous disseminated pulmonary tuberculosis
- 46. Bronchiectasis
- 47. Bronchiectasis
- 48. Broncholithiasis MeduMed.Org - Medicine is Our Vocation
- 49. Chronic bronchitis I stage. MeduMed.Org - Medicine is Our Vocation
- 50. Chronic bronchitis III stage.
- 51. Central lung cancer MeduMed.Org - Medicine is Our Vocation
- 52. Hypoplasia of the left pulmonary artery MeduMed.Org - Medicine - Our Vocation
- Main reasons..." target="_blank"> 53. Hemoptysis and pulmonary hemorrhage
- Main reasons
- 1) Tumors of the lungs (central cancer, bronchus adenoma)
- 2) PE, pulmonary infarction
- 3) Croupous pneumonia
- 4) Pulmonary tuberculosis
- 5) Anomalies of the lungs (AVA, varicose veins)
- 6) Aspergillosis
- 7) Hemosiderosis (congenital, heart disease)
- 54. Algorithm of radiological examination for hemoptysis and pulmonary hemorrhage
- Level I Chest x-ray Source established Not established Peripheral TELA? delayed snapshot
- Level II CT APG
- 55. Tuberculous cavern MeduMed.Org - Medicine is Our Vocation
- 56. Pulmonary Aspergillosis MeduMed.Org - Medicine is Our Vocation
- 57. Varicose veins of the lung MeduMed.Org - Medicine - Our Vocation
- 58. Peripheral cancer in the decay phase
- 59. Abdominal organs MeduMed.Org - Medicine is Our Vocation
- Main reasons
- 1) ..." target="_blank"> 60. Sharp belly
- Main reasons
- 1) Hollow organ perforation
- 2) Intestinal obstruction
- 3) Acute appendicitis
- 4) Cholelithiasis
- 5) Acute pancreatitis
- 6) Abscess of the abdominal cavity
- 7) Renal colic
- 61. Algorithm of radiological examination in acute abdomen syndrome
- Level I Plain radiograph of the abdomen, ultrasound The picture is clear The picture is not clear
- Laterogram
- Level II X-ray contrast study, CT
- 62. Hollow organ perforation MeduMed.Org - Medicine - Our Vocation
- 63. Intestinal obstruction MeduMed.Org - Medicine - Our Vocation
- 64. Right subphrenic abscess MeduMed.Org - Medicine - Our Vocation
- 65. Acute appendicitis
- 66. Thrombosis of mesenteric vessels
- <..." target="_blank">43. Chronic cough
 Methods of X-ray examination of the chest organs: ü ü ü ü ü X-ray; radiography; Longitudinal tomography; Bronchography; CT scan; Magnetic resonance imaging; Angiopulmonography; Radionuclide research; Ultrasound examination of the heart and pleural cavities.
Methods of X-ray examination of the chest organs: ü ü ü ü ü X-ray; radiography; Longitudinal tomography; Bronchography; CT scan; Magnetic resonance imaging; Angiopulmonography; Radionuclide research; Ultrasound examination of the heart and pleural cavities.
 X-ray Objectives: to determine the degree of displacement of shadows during the patient's breathing; ü evaluate changes in the transparency of the lung background during inhalation and exhalation, which makes it possible to judge the elasticity of the lung tissue; ü dynamic control of the pathological process and the level of fluid in the pleural cavity; ü for the purpose of puncture biopsy of formations in the chest cavity. u
X-ray Objectives: to determine the degree of displacement of shadows during the patient's breathing; ü evaluate changes in the transparency of the lung background during inhalation and exhalation, which makes it possible to judge the elasticity of the lung tissue; ü dynamic control of the pathological process and the level of fluid in the pleural cavity; ü for the purpose of puncture biopsy of formations in the chest cavity. u

 Radiography Projections: Ø Direct posterior Ø Lateral left Ø Lateral right Ø Oblique Ø Direct anterior Ø Sighting
Radiography Projections: Ø Direct posterior Ø Lateral left Ø Lateral right Ø Oblique Ø Direct anterior Ø Sighting
 X-ray Imaging of the lungs in direct anterior projection The purpose of the study: to study the state of the lungs in case of suspicion of any of their diseases or damage. Laying for the image: the image is taken in the position of the patient standing (or sitting, depending on the condition) at a special vertical stand; the patient presses his chest tightly against the cassette, slightly bending forward.
X-ray Imaging of the lungs in direct anterior projection The purpose of the study: to study the state of the lungs in case of suspicion of any of their diseases or damage. Laying for the image: the image is taken in the position of the patient standing (or sitting, depending on the condition) at a special vertical stand; the patient presses his chest tightly against the cassette, slightly bending forward.



 X-ray Imaging of the lungs in the lateral projection Produced in the left or right projections. The patient is placed in such a way that he is pressed against the cassette by the examined side. Hands raised up and crossed over the head.
X-ray Imaging of the lungs in the lateral projection Produced in the left or right projections. The patient is placed in such a way that he is pressed against the cassette by the examined side. Hands raised up and crossed over the head.



 Longitudinal tomography Tasks: 1. Determine the nature, exact localization and prevalence of the pathological process in the lung parenchyma; 2. To study the state of the tracheobronchial tree, including, in most cases, segmental bronchi; 3. Clarify the nature of the damage to the lymph nodes of the roots and mediastinum in various pathological conditions.
Longitudinal tomography Tasks: 1. Determine the nature, exact localization and prevalence of the pathological process in the lung parenchyma; 2. To study the state of the tracheobronchial tree, including, in most cases, segmental bronchi; 3. Clarify the nature of the damage to the lymph nodes of the roots and mediastinum in various pathological conditions.


 Bronchography Method of X-ray examination of contrasted large and medium bronchi throughout their entire length after preliminary anesthesia
Bronchography Method of X-ray examination of contrasted large and medium bronchi throughout their entire length after preliminary anesthesia
 Bronchography A plan for studying a bronchogram: For each bronchus, take into account: a) position, b) shape, c) width of the lumen, d) nature of filling, e) angle of departure and nature of branching, f) contours, g) localization and nature of deviations from the normal pattern . In relation to the bronchi, not filled with a contrast agent, take into account the position, shape and outline of their stump, the state of the lung tissue surrounding the bronchi.
Bronchography A plan for studying a bronchogram: For each bronchus, take into account: a) position, b) shape, c) width of the lumen, d) nature of filling, e) angle of departure and nature of branching, f) contours, g) localization and nature of deviations from the normal pattern . In relation to the bronchi, not filled with a contrast agent, take into account the position, shape and outline of their stump, the state of the lung tissue surrounding the bronchi.

 X-ray computed tomography Features of CT-image: ú No superposition; ú Transverse layer orientation; ú High contrast resolution ú Determination of absorbance; ú Various types of image processing.
X-ray computed tomography Features of CT-image: ú No superposition; ú Transverse layer orientation; ú High contrast resolution ú Determination of absorbance; ú Various types of image processing.

 Magnetic resonance imaging A method based on the paramagnetic properties of tissues. Indications: - Volumetric processes in the mediastinum; -assessment of the condition of the lymph nodes; - pathological changes in large vessels; -determination of the germination of lung tumors in the mediastinum, large vessels and pericardium. Restrictions: -calcifications; - evaluation of the lung parenchyma.
Magnetic resonance imaging A method based on the paramagnetic properties of tissues. Indications: - Volumetric processes in the mediastinum; -assessment of the condition of the lymph nodes; - pathological changes in large vessels; -determination of the germination of lung tumors in the mediastinum, large vessels and pericardium. Restrictions: -calcifications; - evaluation of the lung parenchyma.
 Angiography of the lungs is a technique for X-ray examination of the vessels of the lungs after their contrasting with water-soluble iodine-containing non-ionic RCS. Varieties of the technique: ü Angiopulmonography; üSelective angiography of one lung or its lobe (segment); ü Angiography of bronchial arteries; ü Thoracic aortography.
Angiography of the lungs is a technique for X-ray examination of the vessels of the lungs after their contrasting with water-soluble iodine-containing non-ionic RCS. Varieties of the technique: ü Angiopulmonography; üSelective angiography of one lung or its lobe (segment); ü Angiography of bronchial arteries; ü Thoracic aortography.

 Radionuclide study Indications: ú suspicion of pulmonary embolism; ú suspected pulmonary infarction; ú areas with reduced blood flow or its absence are revealed in the form of zones with low-intensity radiation.
Radionuclide study Indications: ú suspicion of pulmonary embolism; ú suspected pulmonary infarction; ú areas with reduced blood flow or its absence are revealed in the form of zones with low-intensity radiation.

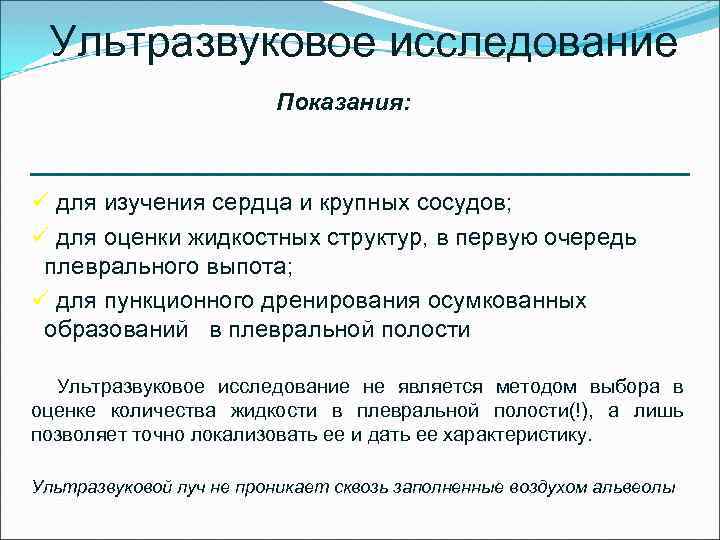 Ultrasound examination Indications: ü to study the heart and large vessels; ü to assess fluid structures, primarily pleural effusion; ü for puncture drainage of encysted formations in the pleural cavity Ultrasound examination is not the method of choice in assessing the amount of fluid in the pleural cavity (!), but only allows you to accurately localize it and give its characteristics. Ultrasonic beam does not penetrate air-filled alveoli
Ultrasound examination Indications: ü to study the heart and large vessels; ü to assess fluid structures, primarily pleural effusion; ü for puncture drainage of encysted formations in the pleural cavity Ultrasound examination is not the method of choice in assessing the amount of fluid in the pleural cavity (!), but only allows you to accurately localize it and give its characteristics. Ultrasonic beam does not penetrate air-filled alveoli
 Normal anatomy of the lungs The lungs are a paired parenchymal organ covered with a visceral pleura. Allocate: 3 shares in the right lung; 2 lobes in the left lung.
Normal anatomy of the lungs The lungs are a paired parenchymal organ covered with a visceral pleura. Allocate: 3 shares in the right lung; 2 lobes in the left lung.


 The functional unit of the lungs is the acinus ü The size of the acinus is up to 1.5 mm. ü Includes alveolar sacs, terminal bronchiole, arteriole, 2 venous branches, lymphatic vessels and nerves. ü A group of acini makes up a lobule.
The functional unit of the lungs is the acinus ü The size of the acinus is up to 1.5 mm. ü Includes alveolar sacs, terminal bronchiole, arteriole, 2 venous branches, lymphatic vessels and nerves. ü A group of acini makes up a lobule.
 Non-parenchymal component 1. Bronchial branches 2. Pulmonary veins 3. Lymphatic vessels 4. Nerves 5. Connecting layers between the lobules, around the bronchi and blood vessels 6. Visceral pleura
Non-parenchymal component 1. Bronchial branches 2. Pulmonary veins 3. Lymphatic vessels 4. Nerves 5. Connecting layers between the lobules, around the bronchi and blood vessels 6. Visceral pleura
 X-ray picture of the chest This is the summation of shadows: - soft tissues of the chest wall - skeleton - lungs - mediastinum - diaphragm
X-ray picture of the chest This is the summation of shadows: - soft tissues of the chest wall - skeleton - lungs - mediastinum - diaphragm
 Soft tissues Muscles - The pectoralis major muscle at the level of 4 m / rib goes obliquely upward and outward and goes beyond the edge of the lung field - Sternocleidomastoid muscle, gives a decrease in the transparency of the lung field in the medial section above the clavicle and passes into the supraclavicular skin fold - Milk gland and shadows of the nipples, darken the lung fields at the level of 4-7 ribs in women and men
Soft tissues Muscles - The pectoralis major muscle at the level of 4 m / rib goes obliquely upward and outward and goes beyond the edge of the lung field - Sternocleidomastoid muscle, gives a decrease in the transparency of the lung field in the medial section above the clavicle and passes into the supraclavicular skin fold - Milk gland and shadows of the nipples, darken the lung fields at the level of 4-7 ribs in women and men
 Bony skeleton The ribs limit the lung fields Above - the lower edge of the posterior section 2 ribs From the sides - shadows of intersecting costal arches In the projection of the lung fields, 11 pairs of posterior sections of the ribs are visible, going first up, then down and out. The front segments stand outside and from top to inside and down. The cartilaginous part of the rib is visible when it is calcified
Bony skeleton The ribs limit the lung fields Above - the lower edge of the posterior section 2 ribs From the sides - shadows of intersecting costal arches In the projection of the lung fields, 11 pairs of posterior sections of the ribs are visible, going first up, then down and out. The front segments stand outside and from top to inside and down. The cartilaginous part of the rib is visible when it is calcified
 Skeleton Shadow of the clavicle It is projected onto the upper parts of the lung fields. With the correct installation of the patient, the inner ends are symmetrically separated from the shadow of the handle of the sternum and spine and are located at level 3 of the intervertebral space.
Skeleton Shadow of the clavicle It is projected onto the upper parts of the lung fields. With the correct installation of the patient, the inner ends are symmetrically separated from the shadow of the handle of the sternum and spine and are located at level 3 of the intervertebral space.
 Skeleton Shadow of the sternum Not visible in frontal projection or partially facets of the manubrium of the sternum from the median shadow. Shadows of the shoulder blades When properly laid, their greater mass is projected outside the lung fields.
Skeleton Shadow of the sternum Not visible in frontal projection or partially facets of the manubrium of the sternum from the median shadow. Shadows of the shoulder blades When properly laid, their greater mass is projected outside the lung fields.
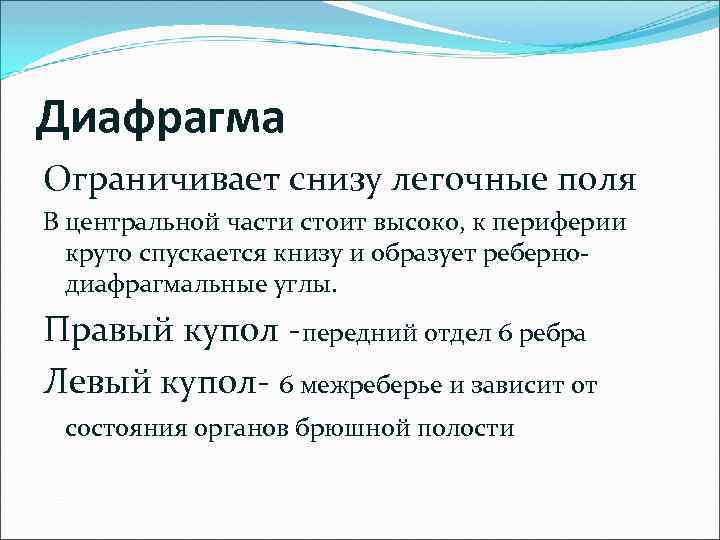 The diaphragm limits the lung fields from below. In the central part it stands high, towards the periphery it descends steeply downwards and forms costophrenic angles. The right dome is the anterior section of the 6th rib The left dome is the 6th intercostal space and depends on the state of the abdominal organs
The diaphragm limits the lung fields from below. In the central part it stands high, towards the periphery it descends steeply downwards and forms costophrenic angles. The right dome is the anterior section of the 6th rib The left dome is the 6th intercostal space and depends on the state of the abdominal organs

 Segmental structure of the lungs The right main interlobar sulcus begins behind the level of 2-3 thoracic vertebra and is projected in the area of the first intercostal space above the shadow of the head of the right root, goes obliquely outward and down towards the rear parts of the ribs and reaches the 5th rib on the lateral outer contour of the chest, anteriorly descends along the anterior end of the 4th rib to the diaphragm (crosses almost in the middle). From the main oblique interlobar sulcus on the right at the level of the 5th rib at the outer contour of the chest, the middle sulcus begins, goes strictly horizontally to the median shadow, crossing the anterior end of the 4th rib along the mid-clavicular line and reaches the middle of the shadow of the arterial part of the root.
Segmental structure of the lungs The right main interlobar sulcus begins behind the level of 2-3 thoracic vertebra and is projected in the area of the first intercostal space above the shadow of the head of the right root, goes obliquely outward and down towards the rear parts of the ribs and reaches the 5th rib on the lateral outer contour of the chest, anteriorly descends along the anterior end of the 4th rib to the diaphragm (crosses almost in the middle). From the main oblique interlobar sulcus on the right at the level of the 5th rib at the outer contour of the chest, the middle sulcus begins, goes strictly horizontally to the median shadow, crossing the anterior end of the 4th rib along the mid-clavicular line and reaches the middle of the shadow of the arterial part of the root.
 Segmental structure of the lungs The posterior border of the left oblique interlobar sulcus is higher, projected at the end of the 1st rib, goes outward more obliquely down and crossing the anterior end of the 6th rib comes to the region of the left cardio-phrenic angle.
Segmental structure of the lungs The posterior border of the left oblique interlobar sulcus is higher, projected at the end of the 1st rib, goes outward more obliquely down and crossing the anterior end of the 6th rib comes to the region of the left cardio-phrenic angle.


 Accessory shares The share of the unpaired vein (lobus venae azygos) Occurs in 3-5% of cases, with an abnormal location of the unpaired vein. If the pleura of the lobe of the unpaired vein is compacted, then it is clearly visible on the direct radiograph on the right in the medial part of the upper lobe. The lingual lobe is analogous to the middle lobe of the right lung.
Accessory shares The share of the unpaired vein (lobus venae azygos) Occurs in 3-5% of cases, with an abnormal location of the unpaired vein. If the pleura of the lobe of the unpaired vein is compacted, then it is clearly visible on the direct radiograph on the right in the medial part of the upper lobe. The lingual lobe is analogous to the middle lobe of the right lung.
 Additional lobes There are other additional lobes: Ø pericardial Ø posterior lobe Additional lobes are ventilated by zonal or segmental bronchi, the number of which is not increased. T. O. with additional interlobar grooves, the amount of lung tissue, bronchi and blood vessels remains normal.
Additional lobes There are other additional lobes: Ø pericardial Ø posterior lobe Additional lobes are ventilated by zonal or segmental bronchi, the number of which is not increased. T. O. with additional interlobar grooves, the amount of lung tissue, bronchi and blood vessels remains normal.





 The shadow of the lungs on the radiograph is called the lung fields. The image consists of a normal lung background and a normal lung pattern. It is important to remember that the lung fields on the radiograph are smaller than the true dimensions of the lung, part of them is blocked by the diaphragm, subdiaphragmatic organs and mediastinum.
The shadow of the lungs on the radiograph is called the lung fields. The image consists of a normal lung background and a normal lung pattern. It is important to remember that the lung fields on the radiograph are smaller than the true dimensions of the lung, part of them is blocked by the diaphragm, subdiaphragmatic organs and mediastinum.
 Pulmonary background This is the degree of blackening of the film within the lung fields. Displays the density of the lung tissue, its air and blood supply.
Pulmonary background This is the degree of blackening of the film within the lung fields. Displays the density of the lung tissue, its air and blood supply.
 Pulmonary drawing Substrate - vessels of the pulmonary circulation. At a young age, the remaining elements of the stroma of the lung are normally not visible. After 30 years, paired strips of thickened bronchial walls appear, the number of which increases with age. This is the age norm. Long linear shadows of blood vessels emanate from the root of the lung, spread like a fan, become thinner and disappear before reaching the periphery 2-2. 5 cm ü Short linear or trabecular shadows - small vascular network ü Looped formations - projection overlay of trabecular shadows ü Small intense focal shadows - these are vessels in a transverse (tangential) section. u
Pulmonary drawing Substrate - vessels of the pulmonary circulation. At a young age, the remaining elements of the stroma of the lung are normally not visible. After 30 years, paired strips of thickened bronchial walls appear, the number of which increases with age. This is the age norm. Long linear shadows of blood vessels emanate from the root of the lung, spread like a fan, become thinner and disappear before reaching the periphery 2-2. 5 cm ü Short linear or trabecular shadows - small vascular network ü Looped formations - projection overlay of trabecular shadows ü Small intense focal shadows - these are vessels in a transverse (tangential) section. u
 Roots of the lungs The anatomical substrate is the pulmonary artery and large bronchi. The image of a normal root is characterized by the presence of structure, i.e., the ability to distinguish its individual elements.
Roots of the lungs The anatomical substrate is the pulmonary artery and large bronchi. The image of a normal root is characterized by the presence of structure, i.e., the ability to distinguish its individual elements.
 Characteristics of the root 1. 2. 3. 4. The position of the root at the level of 2-4 intercostal spaces; Dimensions diameter = 2.5 cm (1:1 pulmonary artery: intermediate bronchus); The outer contour of the pulmonary artery is convex, retracted; Structure - bronchus, artery, vein.
Characteristics of the root 1. 2. 3. 4. The position of the root at the level of 2-4 intercostal spaces; Dimensions diameter = 2.5 cm (1:1 pulmonary artery: intermediate bronchus); The outer contour of the pulmonary artery is convex, retracted; Structure - bronchus, artery, vein.
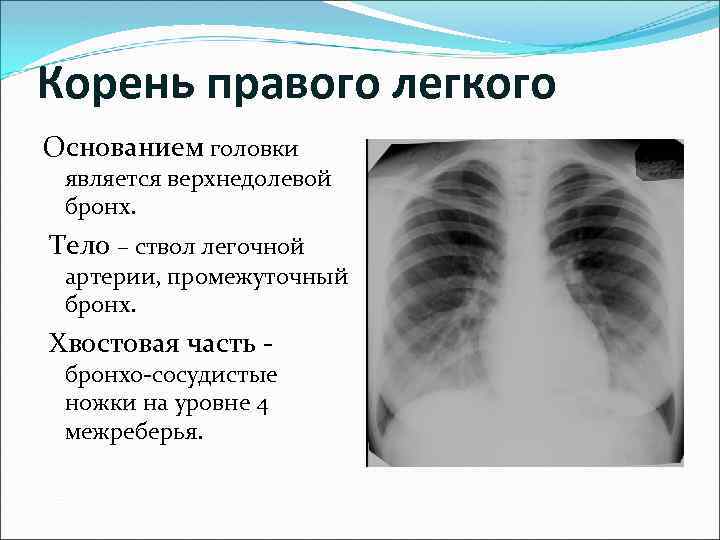 The root of the right lung The base of the head is the upper lobe bronchus. The body is the trunk of the pulmonary artery, the intermediate bronchus. Tail part - broncho-vascular legs at the level of the 4th intercostal space.
The root of the right lung The base of the head is the upper lobe bronchus. The body is the trunk of the pulmonary artery, the intermediate bronchus. Tail part - broncho-vascular legs at the level of the 4th intercostal space.
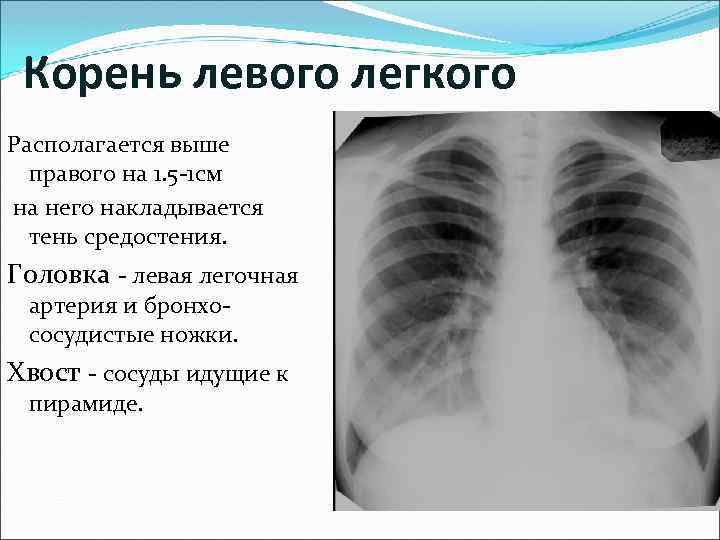 The root of the left lung is located 1.5-1 cm above the right lung, the shadow of the mediastinum is superimposed on it. The head is the left pulmonary artery and bronchovascular pedicles. Tail - vessels going to the pyramid.
The root of the left lung is located 1.5-1 cm above the right lung, the shadow of the mediastinum is superimposed on it. The head is the left pulmonary artery and bronchovascular pedicles. Tail - vessels going to the pyramid.
 Mediastinum Occupies an asymmetric position: 2/3 - in the left chest cavity, 1/3 - in the right. Right contour: § right atrial arch; § ascending aorta; § point of intersection - atriovasal angle.
Mediastinum Occupies an asymmetric position: 2/3 - in the left chest cavity, 1/3 - in the right. Right contour: § right atrial arch; § ascending aorta; § point of intersection - atriovasal angle.
 Mediastinum Left contour: 1 arch - the descending part of the aortic arch, the upper contour is located below 1.5 -2 cm from the sternoclavicular joint; 2 arc - trunk of the pulmonary artery; 3 arc - the ear of the left atrium; 4 arc - left ventricle.
Mediastinum Left contour: 1 arch - the descending part of the aortic arch, the upper contour is located below 1.5 -2 cm from the sternoclavicular joint; 2 arc - trunk of the pulmonary artery; 3 arc - the ear of the left atrium; 4 arc - left ventricle.

 Algorithm for studying radiographs of chest organs. cells 1. Quality assessment 2. 3. 4. Determination of the correct installation of the patient. X-ray anatomical orientation (shape and size of the chest, topography of the organs of the chest cavity). Study of soft tissues and bone skeleton (symmetry, shape, structure)
Algorithm for studying radiographs of chest organs. cells 1. Quality assessment 2. 3. 4. Determination of the correct installation of the patient. X-ray anatomical orientation (shape and size of the chest, topography of the organs of the chest cavity). Study of soft tissues and bone skeleton (symmetry, shape, structure)
 Algorithm for studying chest radiographs Comparison of the transparency of the right and left lungs. 6. Analysis of the lung pattern. 7. Evaluation of the roots of the lungs. 8. Aperture position. 9. The state of the costophrenic sinuses. 10. The study of the organs of the mediastinum. 5.
Algorithm for studying chest radiographs Comparison of the transparency of the right and left lungs. 6. Analysis of the lung pattern. 7. Evaluation of the roots of the lungs. 8. Aperture position. 9. The state of the costophrenic sinuses. 10. The study of the organs of the mediastinum. 5.


 The work used illustrations and materials from the Moscow Humanitarian Faculty of Medicine and Dentistry, as well as materials found on the Internet.
The work used illustrations and materials from the Moscow Humanitarian Faculty of Medicine and Dentistry, as well as materials found on the Internet.
Methods of X-ray examinations of the lungs. X-ray examination of the lungs plays an important role in modern clinical practice. Mostly X-ray examinations are performed.
The primary method of lung imaging is chest x-ray. Chest X-ray is certainly indicated for clinical suspicion of lung disease, chest trauma and polytrauma, in patients with an unclear cause of fever, and oncological diseases.
Radiography is survey and sighting. Overview images, as a rule, should be performed in two projections - frontal and lateral (with the side being examined to the cassette). Plain chest radiographs will always show both the anterior and posterior ribs, collarbone, scapula, spine, and sternum, regardless of the projection of the image (Figures 3.1 and 3.2). This is the difference between a plain radiograph and a tomogram.
Tomography. This technique is the next step in the X-ray examination (Fig. 3.3). Longitudinal direct tomography is more commonly used. The median cut is made at the level of half the thickness of the chest; the middle of the anterior-posterior diameter (from the back to the sternum) in an adult is 9-12 cm.
The anterior cut is 2 cm closer to the median anteriorly, and the posterior slice is 2 cm posterior to the median. On the median tomogram, shadows of either the anterior or posterior sections of the ribs will not be detected, on the anterior tomogram, the anterior sections of the ribs are well visualized, and on the posterior tomogram, on the contrary, the posterior sections of the ribs. Usually, topographic sections of the lungs can be most easily identified by these main features. Longitudinal tomography is used for:
- detailing the topography, shape, size, structure of pathological formations of the larynx, trachea and bronchi, roots of the lungs, pulmonary vessels, lymph nodes, pleura and mediastinum;
- study of the structure of pathological formation in the lung parenchyma (presence and features of destruction, calcification);
- clarification of the connection of the pathological formation with the root of the lung, with the vessels of the mediastinum, chest wall;
- detection of a pathological process with insufficiently informative radiographs;
- evaluation of the effectiveness of treatment.
CT. Computed tomography provides diagnostic information that is unattainable by other methods (Fig. 3.4).
CT is used for:
- detection of pathological changes hidden by pleural exudate;
- assessment of small-focal dissemination and diffuse interstitial lung lesions;
- differentiation of solid and liquid formations in the lungs;
- detection of focal lesions up to 15 mm in size;
- detection of larger foci of lesions with an unfavorable location for diagnosis or a slight increase in density;
- visualization of pathological formations of the mediastinum;
- assessment of intrathoracic lymph nodes. With CT, the lymph nodes of the roots of the lungs are visualized in size, starting from 10 mm (with conventional tomography - at least 20 mm). If the size is less than 1 cm, they are regarded as normal; from 1 to 1.5 cm - as suspicious; larger ones - as definitely pathological;
- solving the same issues as with conventional tomography and its lack of information;
- in case of possible surgical or radiation treatment.
X-ray. Transillumination of the chest organs as a primary study is not performed. Its advantage is real-time image acquisition, assessment of the movement of chest structures, multi-axis examination, which provides adequate spatial orientation and the choice of the optimal projection for targeted images. In addition, under the control of fluoroscopy, punctures and other manipulations on the chest organs are performed. Fluoroscopy is performed using an EOS.
Fluorography. As a screening method for lung imaging, fluorography is supplemented by full-format radiography in unclear cases, in the absence of positive dynamics within 10-14 days, or in all cases of detected pathological changes and with negative data that disagree with the clinical picture. In children, fluorography is not used because of the higher radiation exposure than with radiography.
Bronchography. The method of contrast study of the bronchial tree is called bronchography. The contrast agent for bronchography is most often yodolipol, an organic compound of iodine and vegetable oil with an iodine content of up to 40% (yodolipol). The introduction of a contrast agent into the tracheobronchial tree is performed in different ways. The most widely used methods using catheters are transnasal catheterization of the bronchi under local anesthesia and subanesthetic bronchography. After the introduction of a contrast agent into the tracheobronchial tree, serial images are taken, taking into account the sequence of contrasting the bronchial system.
As a result of the development of bronchoscopy based on fiber optics, the diagnostic value of bronchography has decreased. For most patients, the need for bronchography arises only in cases where bronchoscopy does not give satisfactory results.
Angiopulmonography is a technique of contrast examination of the vessels of the pulmonary circulation. More often, selective angiopulmonography is used, which consists in the introduction of a radiopaque catheter into the cubital vein, followed by passing it through the right cavities of the heart selectively to the left or right trunk of the pulmonary artery. The next stage of the study is the introduction of 15-20 ml of a 70% aqueous solution of a contrast agent under pressure and serial imaging. Indications for this method are diseases of the pulmonary vessels: embolism, arteriovenous aneurysms, pulmonary varicose veins, etc.
Radionuclide studies of the respiratory organs. Methods of radionuclide diagnostics are aimed at studying the three main physiological processes that form the basis of external respiration: alveolar ventilation, alveolar-capillary diffusion and capillary blood flow (perfusion) of the pulmonary artery system. Currently, practical medicine does not have more informative methods for registering regional blood flow and ventilation in the lungs.
To carry out this kind of research, two main types of radiopharmaceuticals are used: radioactive gases and radioactive particles.
regional ventilation. Radioactive gas 133 Xe is used (T½ biological - 1 min, T½ physical - 5.27 days, -, β-radiation). The study of alveolar ventilation and capillary blood flow using 133 Xe is carried out on multi-detector scintillation devices or a gamma camera.
Radiospirography (radiopneumography)
With intratracheal administration, 133 Xe spreads through various zones of the lungs, according to the level of ventilation of these zones. Pathological processes in the lungs, which lead to a local or diffuse violation of ventilation, reduce the amount of gas entering the affected areas. This is recorded using radiodiagnostic equipment. External recording of xenon -radiation makes it possible to obtain a graphical record of the level of ventilation and blood flow in any given area of the lung.
The patient inhales 133 Xe, when a plateau occurs, takes a deep breath and exhale (maximum). Immediately after washing out, the 2nd stage is carried out: an isotonic solution of NaCl with 133 Xe dissolved in it is injected intravenously, which diffuses into the alveoli and exhales.
To assess regional ventilation, the following indicators are determined:
− vital capacity of lungs (VC), in %;
− total lung capacity (TLC); in %,
− residual lung volume (VR);
is the half-life of the indicator.
To assess arterial blood flow, determine:
− amplitude height;
is the half-life of the indicator.
Intrapulmonary dynamics of 133 Xe depends on the degree of participation of the alveoli in external respiration and on the permeability of the alveolar-capillary membrane.
The height of the amplitude is directly proportional to the amount of radionuclide and, consequently, to the mass of blood.
Currently, Technegas is more often used to study the ventilation function of the lungs, which is nanoparticles (5-30 nm in diameter and 3 nm thick), consisting of 99m Tc, surrounded by a carbon shell, which are placed in an inert argon gas. "Technegaz" is inhaled into the lungs (Fig. 3.5.).
Perfusion lung scintigraphy. It is used to study pulmonary blood flow, usually to diagnose pulmonary embolism. The radiopharmaceutical is used - 99m Tc - macroaggregate of human serum. The principle of the method lies in the temporary blockade of a small part of the pulmonary capillaries. A few hours after the injection, the protein particles are destroyed by blood enzymes and macrophages. Violations of capillary blood flow are accompanied by a change in the normal accumulation of radiopharmaceuticals in the lungs.
PET is the best way to detect the prevalence of lung cancer. The study is carried out with radiopharmaceuticals - 18-fluorodeoxyglucose. The application of the method is constrained by its high cost.
Magnetic resonance imaging in the diagnosis of respiratory diseases
The use of MRI is mainly limited to the visualization of pathological formations of the mediastinum and roots of the lungs, lesions of the chest wall, the identification and characterization of diseases of the large vessels of the chest cavity, especially the aorta. The clinical significance of MRI of the lung parenchyma is low.
Ultrasound in the diagnosis of respiratory diseases. This method is of limited value in the diagnosis of most diseases of the chest (with the exception of diseases of the cardiovascular system). With its help, you can get information about the formations in contact with the chest or enclosed in it, about the pleural cavity (fluid and dense formations) and the diaphragm (about movement and shape), as well as about formations located in certain parts of the mediastinum (for example, about thymus).
3021 0
X-ray examination of victims at the slightest suspicion of a chest injury should be considered mandatory. There are practically no contraindications to the use of this method. Even shock cannot be a reason for refusing an urgent X-ray examination carried out simultaneously with anti-shock measures.
The main method that determines the tactics of treatment and further examination of the victim is chest x-ray. In cases requiring urgent surgical intervention, the study, as a rule, is limited to performing radiographs in two projections. In the intensive care unit, a mobile device is used for this purpose, in the X-ray diagnostic room - a stationary type installation. Significantly facilitates the production of x-rays using a special wheelchair, the deck of which consists of an x-ray contrast material and a foam mattress that lifts the patient's body.
Survey pictures on such a gurney are performed without changing the position of the patient, only the tube of the x-ray machine and the cassette are moved. In this case, radiographs made in the later position can be of great diagnostic value, which should be done if the patient's condition allows.
With massive pleural effusions, hematomas, mediastinum, bronchial ruptures, the use of super-exposed chest images is indicated, which are produced with a simultaneous increase in voltage to 80-90 kV and an exposure approximately twice that of conventional survey images. On such radiographs, as a rule, it is possible to trace the lumen of the trachea and the main bronchi. In an emergency X-ray examination, superexposed images can partially replace tomography.
Fluoroscopy
It is not possible to perform chest radiography in case of severe chest trauma in the intensive care unit, which is not equipped with a mobile X-ray television attachment. On the other hand, the transillumination of the organs of the chest and abdominal cavity of the patient, who is in a relatively satisfactory condition, significantly supplements the data obtained from the analysis of radiographs.Transmission should be polypositional, since the more axes of rotation and changes in the position of the patient the radiologist uses, the more anatomical and functional features he finds in the organ under study. To detect small defects in the diaphragm, it is more rational to translucent the patient in the Trendelenburg position. Taking several sips of a water-soluble contrast agent allows you to identify the relief of the displaced organ.
The use of an image intensifier during transmission not only expands the diagnostic capabilities of the method, but also reduces the radiation exposure. X-ray television, X-ray cinematography and videotape recording are very promising in emergency X-ray diagnostics.
Electroradiography differs from conventional radiography in the device of the X-ray detector and the method for detecting a latent image. The time for obtaining an electroroentgenogram on paper takes 2-3 minutes.
Such speed of obtaining information is an undoubted advantage of the method, especially in cases requiring urgent surgical intervention. In addition, on electroroentgenograms of the chest of patients who have received a chest injury, changes in the soft tissues of the chest wall, rib fractures, and the structure of the lung pattern are revealed much better than on plain radiographs. It is hoped that this very promising method will soon find wide application in emergency thoracic surgery.
Lung tomography in emergency X-ray diagnostics is not widely used. The tasks set for the radiologist during an emergency examination can be successfully solved with the help of a superexposed chest x-ray. However, this does not exclude the use of tomography to study the structure of lung formations in the process of dynamic monitoring of patients with lung damage. The method of layered radiography is especially valuable in the diagnosis of intrapulmonary hematomas, mediastinal hematomas.
To determine the structure of the pathological shadow, tomography is used in two standard projections. When studying large bronchi, the tomography projection is chosen based on their anatomical location. When using a tomographic attachment to the domestic X-ray machine RUM-10, tomograms of the lung tissue are produced with a smearing angle of 30%.
Bronchography for urgent radiodiagnosis of ruptures of large bronchi cannot be recommended as a burdensome and unsafe method for the patient.
Since ventilation and hemodynamics are disturbed in traumatic lung injury, it is very promising to use, in addition to radiographs, perfusion radioisotope scanning, which makes it possible to more fully reveal the degree and nature of vascular disorders in the lung.
The perfusion scanning method is based on temporary obstruction of the capillary bed of the lung by a macroaggregate of human serum albumin labeled with 13H. Particles of the radionuclide, lingering in the capillaries, make it possible to reproduce a graphic, planar image of the lungs. The value of the method lies in its simplicity and clarity. According to the information received, scanning can be compared with angiography.
Scanning is performed after intravenous administration of 250–300 μCi of albumin macroaggregate labeled with 131I in 4–5 ml of isotonic sterile sodium chloride solution. The radionuclide is more often injected into the cubital vein of a patient in the supine position at the time of deep inspiration. The horizontal position of the subject provides a more uniform distribution of the substance in the lungs. Scanograms are produced on any of the available scanners, or on a scintillation gamma camera.
Scanograms should be obtained in the anterior, posterior, right and left lateral projections, which makes it possible to clarify the localization and prevalence of the pathological process. By the time of the radioisotope study, the lung should be completely straightened (if there was a pneumothorax), the pleural cavity is dried, i.e., in practice, scanning the lungs in case of injury is possible only on the 5-6th day after the patient is admitted to the hospital.
Very promising is the use of ultrasonic echolocation in the diagnosis of traumatic chest injuries, the expediency of combining which with X-ray methods of examination is indicated by A.P. Kuzmichev and M.K. Shcherbatenko (1975). A certain experience in the use of ultrasonic echolocation (the UDA-724 device with a one-dimensional sensor of pulsed ultrasound with a frequency of 1.76 MHz) for diagnosing chest damage was accumulated in the early 70s [Durok D. I. et al., 1972; Shelyakhovsky M. V. et al., 1972]. However, unfortunately, it has not yet received wide recognition from practical surgeons.
Ultrasound examination is not burdensome for the patient - it is carried out directly at the bedside or in the emergency room. It allows you to differentiate the presence of blood in the pleural cavity from pneumonia, atelectasis, as well as from pleural overlays of an inflammatory nature. If using X-ray examination it is impossible to detect the presence of liquid up to 200 ml in the pleural cavity (and even up to 500 ml in the absence of air), then with the help of ultrasound it is possible to detect liquid with a layer thickness of 5 mm. The dimensions of the echo-free zone correspond to the thickness of the fluid layer in the pleural cavity.
Diagnostic punctures play an important role in the diagnosis of thoracic injuries. With the help of this simple and always accessible method, it is possible to detect the accumulation of blood in the pleural cavities, to detect the presence of pneumothorax, etc. This method is practically safe, of course, subject to well-known rules. In particular, the lower intercostal spaces should not be chosen as the site of the puncture of the chest wall. This is fraught with the danger of damage to the liver, stomach or spleen. By puncturing even the upper level of the fluid and creating a vacuum in the pleural cavity by aspiration, it is possible to clarify the nature of pneumothorax and chylothorax.
Puncture of the pericardial cavity confirms the presence of hemopericardium and prevents cardiac tamponade, giving the surgeon precious minutes to perform the operation.
For recognition of damage to the main respiratory tract, bronchoscopy is of great value. It not only makes it possible to establish the localization and nature of the rupture of the trachea and bronchi, but in some cases it also allows you to determine from which side the integrity of the lung is broken, to identify the cause of airway obstruction, etc. However, while appreciating all the advantages of this method, never we should not forget about the dangers associated with its use in severe closed injuries of the chest.
In cases of tension pneumothorax and mediastinal emphysema, bronchoscopy can be performed only after the elimination of respiratory failure by good drainage of the pleural cavity and mediastinum.
Certain information in case of chest injury is given by thoracoscopy. With a closed chest injury, indications for thoracoscopy arise in the case of hemopneumothorax with lung compression by more than one third, and in the case of penetrating wounds, if a wound of the heart, main vessels, diaphragm is suspected, and also to determine the severity of lung damage [Kutepov S.M. , 1977]. Thoracoscopes have direct and lateral optics. If it is planned to examine the mediastinum or the root of the lung, it is more convenient to use direct optics, with total pneumothorax it is more advisable to use lateral optics [Chervinsky A. A., Selivanov V. P., 1968].
The study is carried out under local anesthesia in the dressing room or operating room, strictly following the rules of asepsis. The sleeve of the thoracoscope is inserted in the fourth-sixth: intercostal space along the anterior or middle axillary line; through the lateral outlet of the sleeve, you can aspirate blood and air from the pleural cavity, which is especially important in the case of tension pneumothorax. For chest injuries, the thoracoscope is usually inserted through the wound. G. I. Lukomsky and Yu. E. Berezov (1967) recommend the following inspection technique.
After the introduction of the thoracoscope into the pleural cavity, it is rotated around the axis in a vertical position, which allows you to examine the surrounding space, finding out the cause of the gas bubble, establishing the presence or absence of pathological formations in the vicinity of the thoracoscope. With extensive pneumothorax, you can examine almost the entire pleural cavity and the organs located in it. First examine the upper part of the pleural cavity.
To this end, the thoracoscope at a large angle in the chest wall is advanced to the apex of the lung, all the while describing semicircles, and the optics should be directed upwards. Then the anterior, inferior and posterior spaces between the lungs and the chest wall are examined, and the position of the lung in relation to the diaphragm is also established. Then, directing the optics downward and medially, they begin to examine from top to bottom towards the diaphragm. After that, the lower edge of the lung at the diaphragm and the diaphragm itself are examined. Then follow up the other edge of the lung towards the apex.
It goes without saying that in the conditions of a specialized) thoracic department, when examining a victim with a severe chest injury, in addition to the listed basic methods and express diagnostic tools, a number of other more complex methods and tools can be used, the number of which is constantly increasing. However, as we have repeatedly noted, it is far from always possible to use this arsenal of means even partially. The severity of the victim's condition forces the surgeon, without wasting a minute, to establish a topical diagnosis of damage already on the operating table.
E.A. Wagner
In recent years, a significant number of victims with chest trauma come to the hospital in a state of alcoholic or drug intoxication. Impairment of consciousness in victims with severe intoxication can create the illusion of a more serious condition.
Symptoms of a chest injury
Analyzing the severity of the victim's condition, it is necessary to pay attention to the mental status. Aggravating, the victim can create a suspicion of a more serious condition in the absence of one, and vice versa, a state of euphoria can give the impression of a satisfactory condition in the presence of internal injuries. To confirm or exclude alcohol or drug intoxication, it is necessary to conduct a blood test, urine for the content of alcohol or other substances that can affect the state of consciousness.
Forced horizontal position, weakness, dizziness, pallor, weakness may indicate or hypovolemia. Forced semi-sitting and sitting position, increased pain when moving to a horizontal position, lack of air indicate a probable penetrating wound and hemopneumothorax. Cyanosis of the face, tension, bulging of the jugular veins, weak pulse, tachycardia in the presence of wounds in the projection of the heart indicate a possible hemopericardium and developing hemotamponade. Severe pallor, moist skin, weakness, tachycardia indicate hypotension due to internal bleeding.
Weakening of breathing during auscultation indicates the presence of air or blood in the pleural cavity. Box sound during percussion indicates pneumothorax, shortening of percussion sound indicates free fluid. The greater the volume of pathological contents in the pleural cavity, the more the lung is compressed, the more the damaged half of the chest lags behind when breathing.
Shortness of breath at rest (RR > 22-25 per minute) with a chest injury is a sign of developing respiratory failure, which is more often associated with tension pneumothorax.
Coughing when the chest is injured is a sign of blood entering the tracheobronchial tree. In the absence of other diseases in which hemoptysis is possible, the presence of blood in the sputum of these victims is an obvious sign of a lung injury.
Tissue emphysema is an important diagnostic feature of penetrating injury. Most often it is localized around the chest wound. The more massive emphysema, the more likely damage to the lung or bronchi. In a number of observations with an obliterated pleural cavity after suffering exudative and inflammatory diseases, after a severe closed injury or surgical intervention, tissue emphysema may be the only sign of a penetrating injury.
In some patients, the diagnosis of a penetrating wound is made when air enters through the wound.
It is necessary to distinguish between one- and two-sided, single and multiple wounds of the chest. The presence of one wound on each side is referred to as a bilateral chest wound. The presence of more than one wound on one side is a multiple unilateral wound.
Wound localization is important in wound assessment. Thus, wounds localized from the parasternal line on the right to the anterior axillary line on the left are potentially dangerous for the heart, and this zone is designated as cardiac. Wounds located below the line starting in the sixth intercostal space along the midclavicular line, connecting with the angle of the scapula, are potentially dangerous in terms of injury to the diaphragm, and the zone is designated as diaphragmatic. Therefore, with wounds localized in the diaphragmatic zone, one should look for clinical ultrasound symptoms of a thoracoabdominal injury, and with a wound in the cardiac zone, the presence of hemopericardium should be excluded.
Thus, at the stage of examination of the victim, it is possible to identify direct or indirect signs of a penetrating wound of the chest, which, together with an assessment of the severity of physiological disorders, can influence the choice of surgical tactics.
Diagnosis of a chest injury
Examination of stable patients takes place mainly in the conditions of the emergency department. For patients admitted to the operating room without examination, diagnostic studies are performed on the operating table. Obligatory diagnostic methods are survey radiography of the chest, chest and abdomen, electrocardiography and the study of hemoglobin, hematocrit, red blood cell count.
Plain radiography in patients with stable hemodynamic parameters should be performed in a stationary radiological room in a standing position in two projections: frontal and lateral. Assess the lung fields, the median shadow, the shadow of the diaphragm, exclude bone pathology. In the presence of foreign bodies of the chest, a polypositional study allows you to accurately localize them.
When using fluoroscopy, an assessment of the pulsation of the heart is carried out. Identification of total shading of the lung field or total collapse of the lung is an indication for transferring the patient to the operating room. If it is impossible to study in a vertical position, a survey radiography is performed in a direct projection lying down and in a direct lateroposition with the wounded side up. This research method allows you to identify, including a small volume.
Ultrasound in the diagnosis of chest trauma
Ultrasound of the chest and abdomen is necessary in the diagnosis of hemothorax and hemopericardium and combined (thoracoabdominal) injuries. The study is carried out according to the FAST and EFAST methodology (Davis, 2005). To increase the sensitivity of ultrasound in the diagnosis of hemothorax up to 100 ml, it is necessary to perform ultrasound both in the supine position and in the sitting position, since the frequency of detecting small hemothorax significantly increases during polypositional examination. The volume of fluid in the pleural cavity is estimated by the degree of divergence of the sheets of the parietal and visceral pleura, determined at the level of the costophrenic sinus along the posterior axillary and scapular lines.
There is a correlation between the volume of hemothorax and the degree of separation of the pleural sheets. The absence of signs of hydrothorax during the initial ultrasound in a victim with a chest injury, performed shortly after the injury, is an indication for re-examination within an hour if surgical intervention is not started within this period of time. The main obstacle to performing ultrasound is widespread tissue emphysema.
In addition to detecting free fluid in the pleural cavity, ultrasound can detect intrapulmonary changes resulting from a lung injury.
Hemopericardium is an indication for emergency transfer of the victim to the operating room. With ultrasound of the pericardium, one should take into account the possibility that normally its cavity may contain serous fluid up to 60-80 ml, which corresponds to 1-4 mm of separation of the pericardial sheets. Another factor contributing to the overdiagnosis of hemopericardium is the separation of the layers of the pericardium, and hemopericardium and associated (thoracoabdominal) injuries.
Computed tomography in the diagnosis of chest trauma
CT among all the listed radiation methods is the most accurate diagnostic method. It is used to localize foreign bodies and clarify injuries along the wound channel in hemodynamically stable patients.
patients with gunshot and stab wounds of the chest. The use of CT allows assessing the volume of hemo- and pneumothorax, determining the depth of the wound channel in the lung and, as a result, avoiding thoracotomy and performing video-assisted thoracoscopic surgery in a significant number of victims. The advantages of CT are speed, the possibility of obtaining objective quantitative indicators. The sensitivity of spiral CT in detecting hemo- and pneumothorax is 100%.
Thus, the use of radiation diagnostic methods makes it possible to detect hemopneumothorax and, depending on the research method, to estimate its volume. The use of CT makes it possible to assess the severity of injuries along the wound channel with high accuracy. Taking into account the state of the victim's hemodynamics, the results of radiation diagnostics and the time elapsed from the moment of injury to admission, a decision is made on the method of surgical treatment.
The article was prepared and edited by: surgeon