Craniotomy or craniotomy is a complex medical operation known in antiquity. It is carried out in special cases when the doctor needs to gain access to the brain and its membranes, the pathologies and vessels that have arisen. Modern medicine makes surgery safer for the patient compared to the past, when it was accompanied by high mortality.
Craniotomy - what is it?

By right, craniotomy is considered one of the most difficult surgical procedures. Bone trepanation implies a violation of the integrity of the cranium, in which an opening is formed, an incision. The operation is performed under local or general anesthesia. The head is secured with a special holder for maximum precision. With the help of a navigation system, doctors expose exactly the part of the brain that is required. Craniotomy is most common in neurosurgery, which is responsible for the surgery of the central nervous system and brain.
Why is craniotomy necessary?
Doctors may need access to the skull, both routinely and urgently, for example, for severe trauma and cerebral hemorrhage. In these cases and others, craniotomy is performed, the indications for which are extensive, but every year they are narrowed due to the emergence of new, sparing methods of treatment. The operation is performed to correct conditions that will cause serious problems without surgery. These include:
- brain tumors (malignant and benign);
- abscess and other purulent processes;
- hematoma, bruise;
- complex head injury;
- hemorrhage;
- vascular aneurysms;
- neurological events such as acute epilepsy;
- malformation of the skull or brain;
- craniotomy in stroke (with hemorrhage).
Craniotomy - types

To eliminate many pathologies, trepanation is used, the types of which are named based on the localization of access to the brain and the method of performing the operation. The bones of the skull (on the vault) are represented by several plastics, covered with the periosteum from above and adjacent to the meninges from below. In case of damage to the periosteum, as the main nourishing tissue, there is a risk of necrosis and bone death. To avoid this, craniotomy is performed by the following methods:
- classical osteoplastic;
- resection;
- for the purpose of decompression;
- conscious operation;
- stereotaxy - a study of the brain using a computer.
Osteoplastic craniotomy
The most famous type of craniotomy, the classic method of opening the skull, during which a small section of the parietal bone is cut out without damaging the periosteum. The sawn piece is connected with the periosteum with the cranial vault. The skin flap on the leg is folded back and after the operation is placed in place or removed. The periosteum is stitched. No bone defect is observed after surgery. Trepanation (osteoplastic) of the skull is divided into two types:
- With cutting out the skin-periosteal-bone flap simultaneously (according to Wagner-Wolf).
- With cutting out a skin-aponeurotic flap, which has a wide base, and then a bone-periosteal flap on a narrow leg (trepanation according to Olivecron).
Decompressive trepanation

One of the methods designed to reduce intracranial pressure and improve the condition (and function) of the brain is decompression craniotomy (DTC) or Cushing's trepanation, named after a famous neurosurgeon. With it, a hole is created in the bones of the skull through which the harmful element that caused the resulting hypertension is eliminated. It can be pus, blood, cerebrospinal fluid, edematous fluid. Negative health consequences after surgery are minimal, and rehabilitation is short-lived.
Resection trepanation
A less favorable prognosis for rehabilitation has a resection operation, craniotomy during it takes place by imposing a milling hole and then expanding it to the required size (for this, nippers are used). The cut off area is removed together with the periosteum without possible restoration. The bone defect is covered with soft tissues. As a rule, this technique is used when trepanning of the posterior cranial fossa is necessary, as well as the treatment of cranial wounds.
Conscious craniotomy

One of the modern methods of surgery is trepanation without anesthesia. The patient is conscious, his brain is not turned off. He is injected with drugs to relax and injected with local anesthesia. Such an intervention is required when the pathological area is located too close to the reflexogenic zones (and there is a danger of damaging it). During the operation, surgeons constantly monitor the patient's condition and organ activity, controlling the process.
Craniotomy - consequences after surgery
Craniotomy has been performed for a long time and successfully, but it is used in extreme cases when the patient's life is in danger. The fear of this operation is justified, because craniotomy can have the most negative consequences and they depend on the complexity of the operation, the patient's age and state of health. Each situation has a risk of complications, and no matter how steps medicine moves forward, it is not possible to make the intervention completely safe. The most common consequences after craniotomy are:
- infectious complication, as in the case of other operations;
- the appearance of blood clots;
- bleeding;
- neurological disorders;
- deformation of the excised area of the bone;
- headache;
- deterioration of vision and hearing;
- paralysis of the limbs.
Coma after trepanation
The most serious complication after craniotomy is a coma. A person can fall into it even before the operation and not leave after all the necessary manipulations have been carried out. When the contraction of the heart does not depend on the activity of the cerebral cortex, the patient's breathing is supported by the apparatus. The patient is warned in advance about the possible consequences of trepanation, including complications in the brain.
Recovery after trepanation
The recovery period after the operation is carried out in the hospital and at home, after discharge. On the first day, the patient moves away from anesthesia, on the second day he is allowed to rise, on the following days (3-7) the basic functions of the body are restored. After a week in the hospital, the staples are removed and the patient is discharged. It does not matter what technique was chosen: osteoplastic trepanation or another. If the manipulation took place without any consequences, the patient will be able to lead a normal life, but subject to certain restrictions:
- refusal to play sports;
- rejection of bad habits;
- abstinence from nervous shocks;
- periodic visits to medical institutions;
- special diet;
- regular walks;
- reducing the likelihood of recurrent hematomas.
Craniotomy is a complex surgical procedure, and various factors can affect its course. But if all medical recommendations are followed, it will be possible to return to normal life in a short time. In the field of correcting complex diseases, craniotomy offers unlimited possibilities, and medical techniques are constantly being improved to ensure a favorable prognosis for patients.
Craniotomy - indications for surgery, all types of its implementation and consequences - Journal and weight loss website
And we also have

All materials on the site were prepared by specialists in the field of surgery, anatomy and specialized disciplines.
All recommendations are indicative and cannot be applied without consulting your doctor.
Craniotomy is rightfully considered one of the most difficult surgical procedures. The operation has been known since antiquity, when they tried to treat injuries, tumors and hemorrhages in this way. Of course, ancient medicine did not allow avoiding various complications, so such manipulations were accompanied by high mortality. Now trepanation is performed in neurosurgical hospitals by highly qualified surgeons and is designed, first of all, to save the patient's life.
Craniotomy consists in the formation of a hole in the bones, through which the doctor gains access to the brain and its membranes, vessels, pathological formations. It also allows you to quickly reduce the increasing intracranial pressure, thereby preventing the death of the patient.
The operation to open the cranium can be carried out as planned, in the case of tumors, for example, and urgently, for health reasons, with injuries and hemorrhages. In all cases, there is a high risk of adverse consequences, since the integrity of the bones is violated, damage to the nerve structures and blood vessels is possible during the operation. In addition, the very cause of trepanation is always very serious.
The operation has strict indications, and the obstacles to it are often relative, since in order to save the patient's life, the surgeon can neglect the concomitant pathology. Craniotomy is not carried out in terminal conditions, severe shock, septic processes, and in other cases it helps to improve the patient's condition, even if there are serious violations of the internal organs.
Indications for craniotomy
Indications for craniotomy are gradually narrowing due to the emergence of new, more gentle methods of treatment, but still, in many cases, it is the only way to quickly eliminate the pathological process and save the patient's life.

decompressive trepanation is performed without intervention on the brain
The reason for decompressive trepanation (resection) diseases become, leading to a rapid and threatening increase in intracranial pressure, as well as causing a displacement of the brain relative to its normal position, which is fraught with infringement of its structures with a high risk of death:
- Intracranial hemorrhage;
- Injuries (crushing of the nervous tissue, bruises in combination with hematomas, etc.);
- Brain abscesses;
- Large inoperable neoplasms.
Trepanation for such patients is palliative procedure, not eliminating the disease, but eliminating the most dangerous complication (dislocation).
Osteoplastic trepanation serves as the initial stage of surgical treatment of intracranial pathology, providing access to the brain, blood vessels, membranes. It is shown at:

osteoplastic trepanation for brain surgery
To remove a hematoma located inside the skull, both resection trepanation can be used to reduce pressure and prevent displacement of the brain in the acute period of the disease, as well as osteoplastic trepanation, if the doctor sets the task of removing the focus of hemorrhage and restoring the integrity of the head tissues.
Preparing for surgery
If it is necessary to penetrate into the cranial cavity, an important place belongs to the good preparation of the patient for the operation. If there is enough time, the doctor prescribes a comprehensive examination, including not only laboratory tests, CT and MRI, but also consultations of narrow specialists, examinations of internal organs. An examination by a therapist is mandatory, who decides on the safety of the intervention for the patient.

However, it happens that the opening of the skull is carried out urgently, and then the surgeon has very little time, and the patient undergoes the necessary minimum of studies, including general and biochemical blood tests, coagulogram, MRI and / or CT to determine the state of the brain and localize the pathological process. In the case of emergency trepanation, the benefits in the form of preserving life are higher than the likely risks in the presence of concomitant diseases, and the surgeon decides to operate.
During a planned operation after six o'clock in the evening the day before, it is forbidden to eat and drink, the patient once again talks with the surgeon and anesthesiologist, takes a shower. It is advisable to rest and calm down, and in case of strong excitement, sedatives may be prescribed.
Before the intervention, the hair is carefully shaved on the head, the surgical field is treated with antiseptic solutions, the head is fixed in the desired position. The anesthesiologist introduces the patient into anesthesia, and the surgeon proceeds to manipulate.
Opening of the cranial cavity can be done in different ways, therefore, the following types of trepanation are distinguished:
- Osteoplastic.
- Resection.
Regardless of the type of surgery planned, the patient should be subjected to general anesthesia (usually nitrous oxide). In some cases, trepanation is performed under local anesthesia with a solution of novocaine. For the possibility of carrying out artificial ventilation of the lungs, muscle relaxants are introduced. The area of the operation is carefully shaved and treated with antiseptic solutions.
Osteoplastic trepanation
Osteoplastic trepanation aims not only to open the cranium, but also to get inside for various manipulations (removal of hematoma and crush foci after injury, tumor), and its end result should be restoration of the integrity of tissues, including bones. In the case of osteoplastic trepanation, the bone fragment is returned to its place, thus the formed defect is eliminated, and a second operation is no longer required.
The burr hole in this type of operation is made where the path to the affected area of the brain will be the shortest. The first step is a horseshoe-shaped incision of the soft tissues of the head. It is important that the base of this flap is at the bottom, since the vessels supplying the skin and underlying tissue pass from the bottom up radially, and their integrity should not be compromised to ensure normal blood flow and healing. The width of the flap base is about 6-7 cm.
After the musculocutaneous flap with aponeurosis is separated from the surface of the bone, it is turned downward, fixed on napkins dipped in saline or hydrogen peroxide, and the surgeon proceeds to the next stage - the formation of the osteo-periosteal flap.

stages of osteoplastic trepanation according to Wagner-Wolf
The periosteum is dissected and exfoliated according to the diameter of the cutter, with which the surgeon makes several holes. The sections of the bone preserved between the holes are cut out with the help of Gigli's saw, but one "bridge" remains intact, and the bone breaks in this place. The bone flap will be connected to the skull by means of the periosteum in the area of the fractured area.
To ensure that the fragment of the skull bone does not fall inward after being placed in its original place, the cut is made at an angle of 45 °. The area of the outer surface of the bone flap is larger than the inner one, and after returning this fragment to its place, it is firmly fixed in it.
Having reached the dura mater, the surgeon dissects it and enters the cranial cavity, where he can perform all the necessary manipulations. After the intended goal has been achieved, the tissues are sutured in reverse order. Sutures from absorbable threads are applied to the dura mater of the brain, the bone flap is returned to its place and fixed with wire or thick threads, the musculocutaneous area is sutured with catgut. In the wound, it is possible to leave a drainage for the outflow of the discharge. The stitches are removed by the end of the first week after surgery.
Video: osteoplastic trepanation
Resection trepanation
Resection trepanation is performed to reduce intracranial pressure, therefore it is otherwise called decompressive. In this case, it becomes necessary to create a permanent hole in the skull, and the bone fragment is removed completely.
Resection trepanation is performed for intracranial tumors that can no longer be removed, with a rapid increase in cerebral edema due to hematomas with a risk of dislocation of nerve structures. The place of its implementation is usually the temporal region. In this zone, the skull bone is located under a powerful temporal muscle, so the trepanation window will be covered by it, and the brain is reliably protected from possible damage. In addition, temporal lobe trepanation provides a better cosmetic result compared to other possible trepanning areas.

At the beginning of the operation, the doctor cuts out the musculoskeletal flap linearly or in the shape of a horseshoe, turns it outward, dissects the temporal muscle along the fibers and cuts the periosteum. Then a hole is made in the bone with a cutter, which is expanded using special bone Luer pliers. This results in a rounded trepanation hole, the diameter of which varies from 5-6 to 10 cm.
After removing the bone fragment, the surgeon examines the dura mater of the brain, which, with severe intracranial hypertension, can be tense and significantly protrude. In this case, it is dangerous to dissect it immediately, since the brain can quickly shift towards the trepanation window, which will lead to damage and wedging of the trunk into the foramen magnum. For additional decompression, cerebrospinal fluid is removed in small portions by means of a lumbar puncture, after which the dura mater is dissected.
The operation is completed by sequential suturing of tissues with the exception of the dura mater. The bone area cannot be put into place, as in the case of osteoplastic surgery, but later, if necessary, this defect can be eliminated with the help of synthetic materials.
Postoperative period and recovery
After the intervention, the patient is taken to the intensive care unit or postoperative ward, where doctors carefully monitor the function of vital organs. On the second day, with a successful postoperative period, the patient is transferred to the neurosurgery department and spends up to two weeks there.

It is very important to control the drainage discharge, as well as the opening during resection trepanation. Swelling of the dressing, swelling of facial tissues, bruising around the eyes may indicate an increase in cerebral edema and the appearance of postoperative hematoma.
Trepanation is accompanied by a high risk of various complications, including infectious and inflammatory processes in the wound, meningitis and encephalitis, secondary hematomas with inadequate hemostasis, inconsistency of sutures, etc.
The consequences of craniotomy can be various neurological disorders with damage to the meninges, vascular system and brain tissue: disorders of the motor and sensory spheres, intelligence, convulsive syndrome. A very dangerous complication of the early postoperative period is the leakage of cerebrospinal fluid from the wound, which is fraught with the addition of infection with the development of meningoencephalitis.
A long-term result of trepanation is the deformation of the skull after resection of a portion of the bone, the formation of a keloid scar in violation of the regeneration processes. These processes require surgical correction. To protect the brain tissue and for cosmetic purposes, the opening after resection trepanation is closed with synthetic plates.
Some patients after craniotomy complain of frequent headaches, dizziness, decreased memory and performance, a feeling of fatigue and psycho-emotional discomfort. Possible pain in the area of the postoperative scar. Many symptoms following the operation are not associated with the intervention itself, but with the pathology of the brain, which was the root cause of trepanation (hematoma, contusion, etc.).

Recovery after craniotomy includes both drug therapy and the elimination of neurological disorders, social and labor adaptation of the patient. Before stitches are removed, wound care is required, including daily monitoring and dressing changes. You can wash your hair no earlier than two weeks after the operation.
For intense pain, analgesics are indicated, in case of seizures - anticonvulsants, the doctor may prescribe sedatives for severe anxiety or excitement. Conservative treatment after surgery is determined by the nature of the pathology that brought the patient to the operating table.
With damage to various parts of the brain, the patient may have to learn to walk, speak, restore memory and other impaired functions. Complete psycho-emotional rest is shown, it is better to refuse physical activity. An important role at the stage of rehabilitation is played by the patient's relatives, who already at home can help to cope with some of the inconveniences in everyday life (taking a shower or cooking, for example).
Most patients and their relatives are concerned about whether a disability will be established after the operation. There is no definite answer. Trepanation in itself is not yet a reason for defining a disability group, and everything will depend on the degree of neurological disorders and disability. If the operation was successful, there are no complications, the patient returns to his usual life and work, then you should not count on disability.
With severe brain damage with paralysis and paresis, impaired speech, thinking, memory, etc., the patient needs additional care and cannot not only go to work, but also take care of himself. Of course, such cases require the establishment of a disability. After craniotomy, the disability group is determined by a special medical commission from different specialists and depends on the severity of the patient's condition and the degree of disability.
Video: decompressive craniotomy in the treatment of TBI
Cancer and brain tumors video
The brain is reliably protected by the bones of the skull, so access to it for both therapeutic and diagnostic purposes is very difficult. The surgical procedure to open the skull is called craniotomy or craniotomy. The name of this operation "craniotomy" consists of two roots and means that it is associated with the formation of a hole ("tomia") in the skull ("cranio").
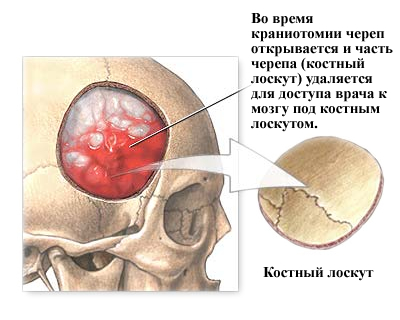
During the surgical procedure for craniotomy, the skull is opened and part of the skull (bone graft) is removed for the doctor to access the brain under the bone graft. The bone graft is usually replaced after the procedure with tiny plates and screws.
Craniotomy can be small or large, depending on the problem. It can be performed during surgery for various neurological diseases, trauma, or diseases such as brain tumors, hematomas, aneurysms, arteriovenous malformations, or skull fractures. Other causes of craniotomy: removal of foreign objects (bullets, etc.), cerebral edema, infections. Depending on the reason for craniotomy, this operation requires the patient to stay in the hospital from several days to several weeks.
A craniotomy is any bony opening that is cut into the skull. There are many types of craniotomy, which are named for specific areas of the skull. Usually the bone flap is replaced. If it is not replaced, the procedure is called "skull removal" or resection.
Craniotomy is also named differently depending on its size and complexity. The small size is called resection trepanation, or "keyhole", because the bony opening is taken out with forceps. Sometimes stereotaxic imaging frames or endoscopes are used to directly accurately insert instruments through these small holes. After resection trepanation, a bone defect remains. If indicated, the postoperative bone defect is closed with various plastic materials.
Keyhole holes for craniotomy are used for minimally invasive procedures:
Inserting a shunt into the ventricles to drain the cerebrospinal fluid (hydrocephalus)
- insertion of a deep brain stimulator for the treatment of Parkinson's disease;
- insertion of an intracranial pressure monitor (ICP);
Removing a small sample of abnormal tissue (biopsy)
- drainage of a blood clot (stereotaxic hematoma);
- removal of intracranial hematomas;
- to reduce intracranial pressure;
- when treating fractures of the skull bones:
- for installing an endoscope when removing small tumors or aneurysms.
Large and complex craniotomy is often referred to as “skull base surgery” or osteoplastic trepanation. These craniotomies involve removing the portion of the skull that supports the lower part of the brain where the delicate cranial nerves, arteries, and veins are located. Reconstruction of the skull base is often necessary and may require additional examination of the head and neck, as well as the work of an otological or plastic surgeon.
Surgeons often use complex craniotomy schemes. A skull base craniotomy can be used to:
Removal or treatment of large brain tumors, aneurysms, or AVMs;
- Treating the brain after a skull fracture or injury (for example, a gunshot wound);
- Removal of tumors that affect the bones of the skull.
When is craniotomy necessary?
The most common indications for a craniotomy are:

Benign and malignant brain tumors;
- bleeding (hemorrhage) as a result of a stroke, trauma or blood clots (hematomas) from trauma (subdural and epidural hematomas);
- weakness in the artery wall (cerebral aneurysms);
- damage to the tissues covering the brain;
- foci of infection in the brain (brain abscesses);
- Severe nerves or facial pain (eg trigeminal neuralgia);
- epilepsy
- removal of foreign objects from the head or brain.
Who performs the craniotomy procedure?
Craniotomy is performed by a neurosurgeon, and some doctors have additional training in skull base surgery. A neurosurgeon can work with the head and neck, an otological surgeon with an ear, an oculoplastic surgeon with eyes and a face.
How to prepare for a craniotomy?
The patient will usually have tests (eg, blood test, ECG, chest x-ray) several days before surgery. In the doctor's office, he signs consent documents and gives full information to the surgeon about his medical history (allergies, medications, reactions to anesthesia, previous operations). The patient should stop all non-steroidal anti-inflammatory drugs (Naproxen, Advil, Ibuprofen, etc.) and blood thinners (Coumadin, Aspirin, etc.) 1 week before surgery. It is also necessary to stop smoking any kind of tobacco and alcohol 2 weeks before and 2 weeks after surgery, because all these actions can lead to serious health problems, including bleeding.
How is craniotomy done?
There are 6 basic steps to craniotomy. Depending on the underlying problem being treated and the complexity, the procedure can take 3 to 5 hours or more.
Step 1 - patient preparation. No food or drink is permitted after midnight on the night before surgery. Craniotomy patients are admitted to the hospital in the morning. General anesthesia is administered intravenously while the patient lies on the operating table. The person falls asleep and their head is in a 3-pin skull fixation device, which is attached to the table and keeps the head upright during the procedure. Inserting a lumbar (cerebrospinal) drain in the lower back helps remove cerebrospinal fluid (CSF), which allows the brain to relax during surgery. The patient may be given a brain-relaxing drug called Manit.
Step 2 - skin incision. After an antiseptic has been applied to the scalp, an incision is made in the skin - usually behind the hairline. The surgeon tries to ensure a good cosmetic result after the operation. Hair can sometimes be shaved gently.
Step 3 - performing craniotomy, opening the skull. The skin and muscles are lifted up to the bone. The surgeon then makes one or more small burr holes in the skull with a drill. By installing a special saw through the burr holes, the surgeon shortens the contour of the bone flap. The cut bone flap is lifted and treated with a protective covering of the brain called the "dura mater". The bone flap is securely stored until it is replaced at the end of the procedure.
Step 4 - brain dissection. After opening the dura mater with surgical scissors, the surgeon puts it back down to expose the brain. Retractors placed on the brain need to be repaired or removed. Neurosurgeons use special magnifying glasses (magnifying glass, or operating microscope) to see fine nerves and blood vessels.
Step 5 - fixing the problem. Due to the fact that the brain is tightly enclosed within the bony skull, the tissues cannot be easily moved to the side, and it is difficult to access them and eliminate all problems. Neurosurgeons use a variety of very small tools to work deep in the brain. These include long-handled scissors, dissectors, drilling rigs, lasers, ultrasonic aspirators (to break up tumors and suck up debris), computerized imaging of targeting systems. In some cases, monitoring is used to stimulate specific cranial nerves while the response is monitored in the brain. This is done in order to preserve the function of the nerves and to make sure that they will not be damaged later during the operation.

Step 6 - Closing the craniotomy. With the problem of removing or repairing retractors, the dura mater, closed with sutures, is also removed from the brain. The bone flap is put back to its original position and is attached to the skull with titanium plates and screws. The plates and screws are permanently retained to support the skull, which can sometimes be felt under the skin. In some cases, drainage tubes may be placed under the skin for several days to remove blood or surgical fluid. The muscles and skin are stitched back together.
The whole procedure takes 180-240 minutes.
What Happens After Your Surgery?
After the operation, the patient is placed in the recovery room, where all of his vital signs are monitored as soon as he wakes up from anesthesia. The breathing tube (ventilator) is usually left in place until the patient fully recovers from the anesthesia. Further, he is transferred to the departments of neurology and intensive care for close observation and monitoring. He will be asked to frequently move his hands, fingers and toes, and legs.
The length of hospital stay ranges from 2-3 days to 2 weeks, depending on the complexity of the operation and the development of any complications. When the patient is discharged from the hospital, he will be given a series of instructions. Stitches or staples are removed 7-10 days after surgery in a doctor's office.
Recovery after craniotomy
Craniotomy is a complex surgical procedure with a relatively long recovery period. Here are some tips that can alleviate the patient's condition after a craniotomy:
- The discomfort. After surgery, the headache is controlled with narcotic drugs. Because narcotic pills are addictive, they are used for a limited period (no more than 2-4 weeks). Eating them regularly can also cause constipation, so you should drink plenty of water and eat foods high in fiber while consuming them. Laxatives (such as Dulcolax, Senocot, Senadexin, Magnesia Milk) can be purchased without a prescription. The pain is then controlled by acetaminophen (eg, Tylenol) and NSAIDs (eg, Aspirin, Ibuprofen, Advil, Motrin, Nuprin, Naproxen, Aleve).
An anticonvulsant may be temporarily prescribed to prevent seizures. Common anticonvulsants: Dilantin (Phenytoin), Tegretol (Carbamazepine), and Neurontin (Gabapentin). Some patients develop side effects caused by these anticonvulsants (eg, drowsiness, problems with balance, rash). In such cases, blood samples are taken to monitor drug levels and manage side effects.
- Restrictions. After a craniotomy, you must not drive until the attending surgeon permits, for an extended period of time. Also, do not lift heavy loads (for example, a 2 liter bottle of water), including children.
In the first weeks after the operation, heavy work at home and in the office is not allowed. This includes: gardening, mowing, vacuuming, ironing, and loading / unloading the dishwasher, washer or dryer.
In no case should you consume alcoholic beverages.
- Activity. Gradually, you need to return to your normal activities. Fatigue is common.
Early Exercise Program - It may be recommended to gently stretch the neck and back. Walking is recommended. You should start with short walks and gradually increase the distance. Do not engage in other forms of exercise without the permission of your surgeon.
- Bathing. The patient can shower with shampoo 3-4 days after surgery. Stitches or staples that remain in place when the patient is discharged should be removed 7 to 14 days after surgery. The patient should ask their surgeon or call the office when this can be done.
- Recovery. Recovery time varies from 1 to 4 weeks, depending on the underlying condition being treated and your overall health. Full recovery can take up to 8 weeks. Walking is a good way to increase your activity level. You should start with short, frequent walks in the house and gradually try to go outside. It is important not to overdo it, especially if the person is continuing radiation or chemotherapy treatments. The surgeon can tell his patient when he can gradually return to work.
Risks and complications of craniotomy (craniotomy)
Any surgical intervention is not without risk. Common complications from any surgery include: bleeding, infection, blood clots, and reactions to anesthesia. There may be specific complications associated with craniotomy: convulsions; cerebral edema, which may require a second craniotomy; nerve damage, which can lead to muscle paralysis or weakness; leaks that may require recovery; loss of mental functions; irreversible brain damage with corresponding disabilities, etc.
Forecast of craniotomy (craniotomy)
The results of craniotomy depend on the underlying disease being treated.
Craniotomy is a complex surgery that involves making an artificial hole in the bone to access the brain. In the process, complications can arise, some of which do not depend on the skill of the surgeon and can lead to disability or death of the patient. And even if everything goes well, recovery after craniotomy will be long and will require the patient to strictly comply with the requirements of the attending physician.
Surgical intervention affecting the brain is so serious that it is carried out in the only case - if not just a person's health is at risk, but his life. Trepanation is prescribed:
- if a neoplasm is maturing in the patient's brain - even if it has nothing to do with oncology, as it grows, it will squeeze the parts of the brain, cause monstrous migraines and hallucinations, making normal life almost impossible;
- if cancer develops in the patient's brain, as the neoplasm develops, it will begin not only to squeeze the adjacent sections, but also to strike them with metastases, which can lead to disability, and later death;
- if an inflammatory infectious process occurs in the patient's brain, the further it goes, the greater the likelihood of irreversible damage that will lead to the failure of certain departments and, accordingly, the functions of the body;
- if the patient's skull was damaged as a result of traumatic brain injury - trepanation can be performed to remove bone fragments, assess the damage and, if possible, compensate for it;
- if the patient has survived a stroke provoked by thrombosis - trepanation is performed to remove a clotted blood clot;
- if the patient suffers from thrombosis and the risk of stroke is very high, trepanation is performed to remove blood clots;
- if the patient suffers from cerebral bleeding, provoked by a sudden rupture of the vessel, trepanation is designed to open the doctor access to the brain and the ability to cope with the bleeding;
- if there is a suspicion of brain cancer and a biopsy is needed, trepanation opens the brain so that tissue samples can be taken from it.
For less serious reasons, trepanation is not performed - while it is possible, doctors always strive to do without such a serious intervention. Their efforts are especially great if the patient's chances of surviving the operation without complications are not very high.
Factors that increase the risk of complications
Craniotomy always comes with a certain risk of complications, but there are factors that can significantly raise it - as well as the risk of complications during the recovery period. To somehow compensate for this, it should be borne in mind that the following are in danger:
- Elderly people. Worn out vessels of the heart and brain can not withstand the load under general anesthesia, reduced vitality and metabolic rate can significantly affect the success of the recovery process, concomitant diseases (and even the healthiest and most successful people develop them by old age) can affect the outcome of the operation.
- Children. The compensatory mechanisms of the child's body are not yet sufficiently developed, as well as his immunity, therefore any surgical intervention poses a significant risk for children. In addition, it is impossible to explain to a small child the need to comply with the regime after craniotomy, he can harm himself.
- People who have already experienced skull surgery in their lives. Often, after the first operation, adhesions are formed between the membranes of the brain and its substance, pressing against the part of the bone that was once opened. With repeated intervention, there is a high risk of damaging the entire structure.
- People suffering from blood diseases. Hemophilia, anemia - any diseases that affect the rate of blood clotting significantly increase the likelihood of bleeding during surgery and add problems in order to somehow compensate for it.
- People suffering from diabetes. Due to the specific features of this disease, all blood vessels are damaged to one degree or another, which greatly complicates the recovery period.
- People suffering from any type of immune deficiency syndrome. If they are present, the likelihood of developing an infectious inflammatory process as a result of surgery increases significantly. If possible, doctors avoid prescribing craniotomy for patients in this group - but if it is still necessary, great efforts are needed to compensate for the disease.

However, even if a person is completely healthy, the recovery process will be long and it will not be possible to insure against the development of complications.
Possible complications
There are two options for complications that can develop in a patient who has been assigned to surgery:
- Early. Their occurrence occurs directly during the intervention and often does not even depend on the skill of the surgeon. Among them:
- Bleeding. Since the brain is abundantly supplied with blood, loss will be rapid and profuse - which is why surgeons always have blood ready for transfusion.
- Damage to the medulla. At the current level of development of medicine, they are rare, but they can lead to a complete failure of the affected area of the brain.
- Edema. It is to them that the brain reacts to any emergency situation. With inaccurate trepanation, the medulla may shift to the area of intervention - often with pathologies and ruptures.
- Death. It can develop for a variety of reasons, up to a simple cardiac failure due to anesthesia and the resulting overload.
- Late. Their occurrence should be expected after trepanation, during the recovery period. They can be provoked by non-observance of the doctor's recommendations, not carefully performed operation and weakness of the body after the intervention. Among them:
- Wound infection. If the hygiene standards were not followed strictly enough, there is a chance that the edges of the wound will become inflamed and swollen, causing pain to the patient.
- Brain infections. They are very rare, but have dire consequences, provoking forgetfulness, irreversible personality changes, seizures, and refusals of certain departments.
- Blood clots and blood congestion. After the operation, a person usually moves a little, therefore there is a high likelihood of thrombosis, which already threatens with its complications, up to strokes and heart attacks.
- Neurological disorders. The brain tissue can swell, which will disrupt the work of its departments. A person can have problems with everything from speech to coordination - permanent or temporary, depending on the extent of the lesion.
Also, the patient may feel depressed, have problems with sleep and appetite, suffer from impaired speech and coordination, may become irritable or whiny. The main thing is to carefully monitor any suspicious symptoms and, while rehabilitation after craniotomy lasts, carefully inform your doctor about them.
There are no unimportant symptoms - if something causes anxiety in the patient, you need to talk about it.
The recovery period in the hospital
Even if the operation was completely successful, the patient is left in the hospital for observation and compensation of the consequences of the intervention for a week. During this time:
- On the first day. For the first few hours, while the patient is recovering from anesthesia, an oxygen mask remains on him, catheters are connected to the arm, which record the pulse and supply a nutrient solution to the vein, and a sensor to the head that records intracranial pressure. As soon as the patient wakes up, the doctor assesses his general condition, how well he is with coordination, whether he is adequate. The mask is removed, and the catheters are also removed.
- On the second day. The patient is allowed to get up and independently get to the toilet. The drainage is removed, it is allowed to take food on his own, if the patient feels capable of it. His face is still bruised and swollen.
- On days three to seven. The patient restores the basic functions of the body, bruises and swelling slowly disappear, doctors closely monitor his condition. If there are suspicions of complications, they try to stop them at the very beginning.
- On the seventh day. The staples that remained after trepanation are removed and, having given the patient all the necessary instructions, they are discharged home.

All the time, while the recovery after the craniotomy operation is underway, the patient can receive the following medications:
- pain relievers - they allow you to relieve constant pain in a head wound;
- anti-inflammatory - they reduce the likelihood of developing infectious complications to almost a minimum;
- sedatives - they allow the patient to provide a constant calm and even mood, which is useful, because he cannot be nervous;
- anticonvulsant and antiemetic - they can save the patient from unpleasant side effects;
- steroid - they remove unnecessary water from the body, which leads to a decrease in pressure.
In addition, every day the wound is cleaned, which is necessary so that it does not become inflamed and fester. In addition to medicines, the patient is usually prescribed:
- Diet. A weakened body must spend all its energy on recovery, and not on digesting food, therefore, in the first week, hospital food is usually as easy as possible to digest. Boiled and mashed potatoes, compotes and jelly, a little bread. Often the combination of drugs can cause constipation in the patient, and then he is advised to drink more.
- Breathing exercises. With a sedentary lifestyle, the lungs always suffer, therefore, from the very first day, the patient is shown a set of exercises that he must perform while lying down - usually these are various inhalations and exhalations.
In the first week, you can not actively move and be nervous. Only rest and medical supervision allow you to recover enough for discharge.
Recovery period at home
Even after a successful operation, you need to pay a lot of attention to the recovery period - it should last at least six months. Should:
- Give up bad habits - they can provoke problems.
- Do not lift weights - loads over three kilograms are completely contraindicated.
- Refrain from nervous excitement - if it does not work out, you should drink a course of soothing herbs. If they do not have an effect, this may be evidence of a developing neurological disease and you should consult a doctor.
- Refrain from bending down - if you need to lift something, it will be better to sit down.
- Walking every day, at a not too fast pace. It is advisable to choose a quiet, calm place for walking, away from the bustle of the city. A shady park or small grove will do.
- Eating a diet - Eating well is essential for a healthy recovery.
If the craniotomy is successful, the recovery period allows the patient to return to full life in a relatively short time. The main thing is to listen to the doctor, monitor your health and take your time.
Despite the fact that mankind does not know everything about the brain, neurosurgery has achieved great success in our time. But no matter how high the level of brain surgery, the phrase "craniotomy" evokes unpleasant associations in most people. However, this complex and lengthy surgical procedure saved many lives. You can familiarize yourself with the indications for such an operation, its types and possible consequences in this article.
Historical reference
In neurosurgery, trepanning is the punching of a hole in some part of the skull to access directly the tissue in the brain. However, such an operation should not be considered an invention of modern medicine. Archaeological finds indicate that our ancestors could have drilled holes in the skull for therapeutic purposes several thousand years ago. Since the late Paleolithic era (40-11 thousand years ago), trepanation has been used in almost all corners of the planet. The operation was used by ancient Greek and Roman doctors, healers in several parts of Africa, South America and the South Pacific.
Hippocrates proposed trepanation as a way to treat head wounds, including the removal of bone fragments from the brain after trauma. For this procedure, his followers came up with a special drill. Prehistoric trepanation in the culture of ancient civilizations of Peru was performed with a ceremonial knife called tumi. Residents of the South Pacific Ocean performed surgery using sharply sharpened shells. In Europe, flint and obsidian were used for the same purposes.
The purpose of trepanation was not always to open access to the brain for further manipulation. In ancient times, a hole in the skull often served as an outlet for evil spirits, who were believed to be the cause of disease. Also, the hole in the skull seemed to be a kind of channel for obtaining special knowledge and spiritual experience. In Egypt, the pharaohs underwent such an operation, presumably to make it easier for the soul to leave the body after death.
Despite the lack of proper sanitary conditions and drug rehabilitation after craniotomy, in many cases, patients of prehistoric surgeons managed not only to survive, but also to live with a hole in the head, closed only by a strip of skin, for many years.
Types of trepanation and indications for them
In modern medicine, craniotomy is also called craniotomy (but not brain trepanation). The other name does not change the fact that this is a very difficult surgical procedure. The emergence of new methods of dealing with many diseases of the brain makes it possible to resort to it less often than before. However, two types of such operations on the skull still take place in neurosurgical practice - osteoplastic, resection trepanation.
Features of osteoplastic craniotomy
Trepanation is done when you need to access directly the contents of the skull for surgical treatment:
The operation begins with choosing a site for the burr hole: it should be as close to the affected area as possible. First of all, the surgeon cuts the soft tissue in the shape of a horseshoe in such a way that the base of the flap is located in the lower part, since the blood vessels pass from the bottom up, and it is very important not to violate their integrity. Further, with the help of special instruments, the periosteum and bone are dissected at an angle of 45 °. Such a cutting angle is needed so that the outer surface of the bone flap exceeds the inner one, and when restoring the integrity of the skull, the removed fragment does not fall inward. Having reached the meninges, the surgeon performs manipulations directly in the cranial cavity (removes the tumor, eliminates hemorrhage).
The craniotomy ends with suture:
- the dura mater is sutured with absorbable sutures;
- the flap is fixed with special threads or wire;
- the skin and muscles are sutured with catgut.

Carrying out resection trepanation
The pretexts for carrying out a resection craniotomy are pathologies that provoke a rapid increase in intracranial pressure, threatening life, or contributing to the displacement of brain structures, which is fraught with their infringement and death. These conditions include:
- cerebral hemorrhage;
- swelling of the brain;
- trauma (bruises, hematomas, crushing of tissues as a result of a blow);
- large inoperable tumors.
Trepanation in such cases is a palliative procedure, that is, it does not eliminate the disease, but only eliminates a dangerous complication.
A resection craniotomy of the skull is also called a decompression craniotomy, since it is performed to reduce the pressure inside the skull. Its peculiarity is that the bone fragment is not returned to its place. If the threat to life disappears over time, the hole can be closed with synthetic material.
The best location for surgery is in the temporal lobe. Here the lining of the brain after removal of the bone flap will be protected by a powerful temporal muscle.
How is craniotomy done? As with osteoplastic craniotomy, soft tissue and bone are cut. The bone fragment is removed so that the diameter of the hole is 5 - 10 cm. Having found swelling of the lining of the brain, the surgeon is in no hurry to dissect it so that the brain structures do not shift. To eliminate intracranial hypertension, you first need to do several punctures of the cerebrospinal fluid, and then cut the lining of the brain. When this manipulation is performed, the tissues (with the exception of the dura mater) are sutured.
Any type of craniotomy can take several hours and is only used for serious indications that threaten the patient's life. No one will do such an operation, for example, with a microstroke - to eliminate its consequences, there are more gentle methods of therapy.
Contraindications to trepanation are terminal conditions (severe shock, extreme coma), septic processes.

Possible complications
The operation is performed under general anesthesia, in some cases, part of the intervention takes place under local anesthesia, that is, the person is conscious. After trepanation, the patient is admitted to the intensive care unit or recovery room. When the patient comes to his senses without incident, he is transferred to the neurosurgery department, the duration of stay there is about 2 weeks.
The consequences of trepanation (anesthesia) can be thirst, headache, but this is not critical. But swollen tissues of the face, bruising around the eyes may indicate the progression of cerebral edema. There are a number of other possible complications after this surgery.
- The course of inflammatory processes in the wound, encephalitis, meningitis is a consequence of the introduction of infections.
- Neurological disorders (seizures, problems with coordination of movements, disorders of the intellectual sphere) are associated with damage to the meninges and tissues.
- Deformation of the skull after removal of a part of the bone, the formation of a keloid scar.
Unpleasant consequences after craniotomy (headaches, dizziness, memory impairment) may be associated not so much with the operation itself, but with a brain disease, due to which the intervention was carried out.

Recovery process
The rehabilitation period after craniotomy lasts different times, depending on the pathology of the brain. At first, you need careful care of the wound, control of the condition of the seams. Intense pains are relieved by analgesics, severe anxiety by sedatives. The patient is recommended physical and emotional rest - the doctor will say how long it is not allowed to go to work.
Your doctor may recommend a diet for quicker recovery. Most likely, you will have to switch to proper nutrition, giving up foods that increase blood pressure and clog blood vessels with cholesterol. We are talking about caffeinated drinks, alcohol, fatty, fried foods.
If the disease has led to damage to some parts of the brain and functional disorders, trepanation is not able to instantly put everything in order. In such situations, rehabilitation may include the need to re-learn to walk, talk, etc.
If a brain disease has led to irreversible processes, and a person is not able to serve himself, he is assigned a disability group. However, the craniotomy itself is not a reason for determining disability if the patient continues to live as before the operation.
