Ulcerative colitis (UC) is a very serious and complex disease of the gastrointestinal tract, which is accompanied by the appearance of ulcers on the mucous membrane of the colon. In its advanced form, it is very difficult to treat it. In addition, it greatly complicates a person's life, depriving him of sleep and rest.
The main reasons for the appearance of the disease include hereditary predisposition; transferred infectious diseases; diseases of the gastrointestinal tract; poor environmental situation; emotional instability.
 People with this disease complain of bloody, purulent or mucous discharge. In the case of a severe course of the disease, the frequency of stool can reach twenty times a day. As a rule, the urge becomes more frequent at night.
People with this disease complain of bloody, purulent or mucous discharge. In the case of a severe course of the disease, the frequency of stool can reach twenty times a day. As a rule, the urge becomes more frequent at night.
In addition, fever appears, painful sensations in the epigastrium, which intensify after eating. A patient with ulcerative colitis loses a lot of weight.
If you do not seek the help of a specialist in time, intestinal bleeding, rupture of the colon wall, formation of abscesses and fistulas, and narrowing of the intestinal lumen may occur.
The disease can take on a chronic form, which, unfortunately, is very difficult to cure.
Ulcerative colitis: stages
The disease is divided into several stages.
- Chronic. The development of this stage provokes untimely treatment.
- Sharp. The manifestation of the primary symptoms of the disease is characteristic.
- Recurrent. An improvement in the condition is accompanied by an exacerbation.
Forms of the disease
- Lightweight.
- Medium severity.
- Heavy.
The mild form of the disease is characterized by a satisfactory condition, the appearance of no more than five times, sometimes with bloody discharge. In severe cases, fever appears, loose stools become more frequent, blood, purulent and mucous discharge appear.
What does everyone need to know?
 Quite often in scientific publications or on television you can find ulcerative colitis and "walking by the arm." For some reason, many believe that these two diseases are almost identical. Unfortunately, this opinion is extremely erroneous. Of course, there are similar symptoms between ailments, but there are much more differences.
Quite often in scientific publications or on television you can find ulcerative colitis and "walking by the arm." For some reason, many believe that these two diseases are almost identical. Unfortunately, this opinion is extremely erroneous. Of course, there are similar symptoms between ailments, but there are much more differences.
It is characterized by the presence of ulcers only on the mucous membrane of the colon. But with Crohn's disease, ulcers are formed both on the mucous membranes of the large and small intestines. In addition, they can appear in the stomach. Hence it follows that the treatment of these "adjacent" ailments is different.
Therefore, in any case, do not self-medicate, and if suspicious symptoms appear, immediately go to the hospital. With the wrong treatment, you can only aggravate the situation.
Nyak treatment with folk remedies
Drug therapy can bring only a slight improvement, therefore, in this case, the treatment of the disease with the help of traditional medicine is considered the most effective. Correctly selected herbal medicine and helps to alleviate the course of the disease. This is the only treatment in most cases.
Therapy with medicinal plants is the "golden mean". Especially in the case when medications are powerless against this disease, and it is too early to carry out the operation.
List of the most effective medicinal plants
Medicines from plants should have a wound healing and hemostatic effect. In addition, they should help to replenish the water-salt balance in the body.
- Blueberries help cleanse the intestines of putrefactive substances and help fight cancer cells.
- Raspberry and strawberry leaves are the best helpers of the liver in the "battle" with the disease.
- Nettle leaves improve blood clotting.
- Chamomile flowers have powerful antimicrobial and antibacterial properties.
- Yarrow helps cleanse the intestines of harmful microorganisms and stop diarrhea.
- Cinquefoil has a wound healing effect.
- With the help of drugs from sleep, you can relieve inflammation, painful sensations, and cope with constipation.
- Celandine will tidy up the nervous system, help in the fight against microorganisms harmful to humans, and eliminate the inflammatory process.
- With the help of funds from St. John's wort, you can restore intestinal motility.
- Alder has an astringent and wound healing and hemostatic effect.
Chronic stage of ulcerative colitis: treatment
People with this ailment are often worried about stool problems. And therefore, in the treatment of this disease, a bias must be made to these features. Colitis, which is accompanied by diarrhea, must be treated with those medicinal plants that have a strengthening property.
 Preparation of the fastening infusion. You need to take chamomile, yarrow, nettle, St. John's wort and rose hips. Yarrow should be five parts, all other plants one at a time. An infusion from such a herbal collection has an antibacterial and hemostatic effect, helps to eliminate diarrhea.
Preparation of the fastening infusion. You need to take chamomile, yarrow, nettle, St. John's wort and rose hips. Yarrow should be five parts, all other plants one at a time. An infusion from such a herbal collection has an antibacterial and hemostatic effect, helps to eliminate diarrhea.
Stir all the ingredients thoroughly and cover them with a glass of water. Place in a water bath for 15 minutes. Remove from heat and leave to infuse for a couple of hours. Drink one glass of infusion before sitting at the table.
If the disease is accompanied by constipation, then it is necessary to use plants that have a laxative effect.
Laxative infusion recipe
You will need chamomile, creepy, valerian root, nettles, blueberries, and mint. Three tablespoons of raw materials must be poured with boiled water and left to infuse overnight. Take a glass of the product before meals.
Acute stage - treatment
The use of strong brewed green tea will help treat this stage. It has antimicrobial effects. It is recommended to drink large leaf tea.
Preparation of chamomile infusion
One of the most effective plants for treating the acute stage is chamomile. Take four spoons of raw materials and cover with water. Put in a water bath for half an hour, then strain. Consume half a glass of infusion after each meal.
St. John's wort infusion is an excellent remedy for stopping diarrhea in acute attacks.
Take one spoonful of the plant and fill it with a glass of boiled water. Insist for thirty minutes. Drink 1/3 cup before each sitting at the table.
Recurrent colitis
In the period of relapses, it is necessary to use fees that promote increased blood circulation and rapid healing of ulcers. In addition, you need to take funds from those plants that can improve blood clotting. These include: nettle, St. John's wort, lamb and mountaineer pepper. These plants can be added to other medicinal herbal teas.
Sea buckthorn enemas. For any form and any stage of the disease, the use of enemas is quite effective. It has a wound healing and regenerating effect. Take 50 ml of oil in a small medical pear. Then insert it into the rectum. It is advisable to put an enema before going to bed. Take one spoonful of oil in the morning.
Other effective remedies
- Take dried raspberry leaves and fill them with boiled water. Leave to infuse for 30 minutes. Consume 100 ml of the product four times a day before meals.
- Take mint leaves and cover them with boiled water. Let it brew for about 20 minutes. Take a glass of infusion half an hour before sitting at the table.
- For the next preparation, you will need fresh pomegranate seeds. Take 50 g of seeds, cover them with a glass of boiled water and put on low heat for 30 minutes. Drink a decoction of 2 tablespoons twice a day.
Never let this ailment take its course and do not hope that everything will go away by itself. Only through timely and regular treatment can you weaken the course of the disease and prevent serious complications from occurring.
You probably thought that I lost my mind and would begin to offer you some anti-scientific methods of treating ulcerative colitis ... I hasten to clarify: I personally know people who, being without medication support, for 8-10 years and did not remember about their NUC ... However, as you may have guessed, even after such a long period of time, the disease can manifest itself.
Can a ten-year remission of NUC be mistaken for healing? How can you help your body to accomplish the seemingly impossible: to exist safely without medication for many years
Introduction
"I cured the NUC!" - Is this what you want to hear in a dialogue with any patient with IBD? You can disagree with me, however, here is my opinion. If you manage to stay in remission without medication for at least 6-12 months, then you have somehow managed to balance your immune system. We know that the source of NUC lies in the autoaggression of the immune system (the question is, what caused the failure of the immune system, but this is not about that now). Can we assume that after an indefinite time our body will be attacked by some irritant, and ulcerative colitis will again make itself felt? Of course. Can we extend the time of stay in remission, feeling like a healthy person? Of course, but this will take a lot of effort. This is what today's article will be about.
If you, like me, want to fully live the time allotted to you, then everything that you see below in the text must be introduced into your everyday life, because the benefits of all this with NNC have scientific justification.
Manage stress
Stress is not just anxiety or nervous tension, as is commonly believed. Stress is a universal response to sufficiently strong external and internal stimuli. At the same time, every living thing has a so-called endurance threshold... That is, in order for the body to launch a chain of reactions, stress must overcome this very threshold.
The author of this theory (“stress theory”) is Professor Hans Selye. The concept was approved by many scientists and was reflected in scientific and pseudo-scientific publications. According to the canon, stimuli are divided into two types - physical and psychological... The former include extreme ambient temperatures, trauma, illness, etc., the latter include fear, hatred, worries, etc.
By itself as a mechanism “Stress” is negative and positive... I am sure that the overwhelming majority of people at least once in their life had the opportunity to feel the sharpening of reflexes during any extreme situation (I touched on this topic in my article on). This is the "bright side" of stress - eustress... You and I need to pay attention to distress- the "dark side" of this phenomenon (Luke, I am your father: D).
Distress is a condition of a living organism in which it cannot adequately respond to stimuli. Excessive stress, unbalancing you, leads to a deterioration in psychophysiological functions. The body's reserves are not unlimited, and if you stay in a state of distress for too long, there is a high risk of harmful consequences.
Causes of distress include:
- The inability to satisfy their physiological needs (food, drink, heat, oxygen) for a long time.
- Abnormal living conditions (i.e. different from the usual habitat).
- Prolonged pain, injury, illness.
- Long-term negative emotional influences.
Distress leads to disruptions in the hormonal, immune, genitourinary, digestive and other systems of the body, as well as to disturbances in the functioning of various internal organs, including the stomach, small intestine, large intestine, brain, heart, etc. Is it worth telling why this can lead to?
The conclusion from all of the above suggests itself: you must learn to manage your stress... I highly recommend that you read the translation of the article ““. By the way, it is rumored that by repeating the mantra "I have cured ulcerative colitis", some actually succeeded;)
Diversify your diet
Our body is a complex system of interconnection of everything and everyone. To keep the processes in proper condition, they need food.
By limiting ourselves in this or that food, we deprive our body of the opportunity to receive the necessary nutrients (of course, I do not mean fast foods and other obviously harmful products). Read more about the benefits of vitamins - in the articles "" and "".
Focus your attention on eating protein-containing foods such as eggs, chicken, turkey, fatty fish, cottage cheese, and others like them. Protein is the basis for the synthesis of new cells and the repair of damaged ones.
Observe the regimen
You have to teach your body to live “on schedule”. Wake up and fall asleep at the same time, go to the bathroom, eat, exercise, etc. - that's what I mean.
With the current rhythm of life, it can be very difficult to develop the habit of “observing the regime” in oneself due to, for example, irregular working hours or frequent business trips. However, how about that for example eating at a set time reduces the risk of onset and exacerbation of gastrointestinal diseases?
As for myself, I can say that for 2-3 years I have been going to the toilet in the morning, around 6: 30-6: 40. I don’t know, to be honest, how it happened, but this need taught me to wake up around 6:30 in the morning, even on a weekday, even on a weekend. In the gym, I train from 18:00 to 19:00. Meals.
Ulcerative colitis is a chronic inflammatory process on the mucous membrane of the colon, accompanied by the appearance of non-healing ulcers, areas of necrosis and bleeding. This pathology differs from simple inflammation. With it, ulcerative defects form on the mucous membrane of the colon. Prolonged illness increases the likelihood of developing cancer.
Therefore, at the slightest suspicion of this ailment, you should consult a doctor who will recommend the correct treatment of ulcerative colitis with drugs and folk remedies.
What is ulcerative colitis?
Ulcerative colitis of the intestine is a chronic inflammatory disease of the mucous membrane of the colon resulting from interactions between genetic and environmental factors, characterized by exacerbations. UC affects the rectum, gradually spreading continuously or immediately invading the rest of the colon. It is also called ulcerative colitis (NUC).
Usually occurs in adults aged 20 to 35 years or after 60. In children, this disease occurs extremely rarely and accounts for only 10-15% of all identified pathologies. At the same time, girls are at the greatest risk of developing the disease among adolescents, and in the preschool and primary school period, on the contrary, boys.
Ulcerative colitis is classified:
- according to the clinical course - typical and fulmic; chronic form (recurrent and continuous);
- localization - distal (proctitis, proctosigmoiditis); left-sided (up to the middle of the transverse colon); subtotal; total (pancolitis); total with reflux ileitis (against the background of total, the ileum is involved in the process);
- the severity of clinical manifestations.
The pathological anatomy (morphological substrate of the disease) of ulcerative nonspecific colitis is represented by a diffuse superficial lesion of the walls of the large intestine. In the vast majority of cases the disease is localized in the terminal (end) sections of the large intestine: sigmoid and rectum. The defeat of the entire large intestine is much less common. The defeat of the end part of the small intestine is very rare.
Causes
Unfortunately, the exact etiology of this disease is unknown - scientists managed to find out that the autoimmune process, genetic inheritance and certain infectious agents play a role in the formation of the disease.
Ulcerative colitis is more susceptible to residents of cities in developed countries. As a rule, the disease develops either in young people or in those over 60, although in fact a person of any age can get the disease.
It has been suggested that it can be provoked by:
- some unknown infection (but ulcerative colitis is not contagious);
- unbalanced diet (fast food, diet with a lack of fiber, etc.);
- genetic mutations;
- medicines (non-hormonal anti-inflammatory drugs, contraceptives, etc.);
- stress;
- shifts of intestinal microflora.
Under the influence of these factors, symptoms of ulcerative colitis develop as a result of autoimmune processes in the body.
The symptoms of ulcerative colitis of the intestine
Ulcerative colitis has an acute phase and a remission phase. The disease begins gradually at first, but quickly gains momentum when the symptoms become more pronounced.

Digestive system symptoms of ulcerative colitis:
- cramping pain in the abdomen with localization mainly on the left, which is difficult to relieve with drugs;
- diarrhea or loose stools mixed with mucus, blood, or pus, worse at night or in the morning;
- constipation replacing diarrhea, which is caused by intestinal spasm;
- bloating ();
- frequent false urge to defecate (tenesmus), arising from the retention of feces above the area with inflammation;
- spontaneous secretion of mucus, pus and blood (not during the act of defecation) as a result of imperative (irresistible) urges.
In 10% of cases, in addition to the mentioned intestinal and general symptoms, extraintestinal manifestations occur:
- articular lesions;
- various rashes on the skin and mucous membranes (for example, in the mouth);
- eye disorders;
- damage to the liver and bile ducts;
- thrombus formation, etc.
They can precede intestinal disorders. The severity of extraintestinal manifestations sometimes depends on the activity of the inflammatory lesion of the intestine, and in some cases it is completely unrelated to it.
With a mild degree of ulcerative colitis, patients complain of cramping pains or abdominal discomfort, weakness. A semi-liquid stool is possible 2-4 times a day with a small admixture of blood and mucus.
If ulcerative colitis is more severe, then loose stools are up to 8 times a day with a significant admixture of mucus, blood and pus. With this form of the disease, the following are noted:
- pain in the abdomen, more often in the area of its left half (flank).
- there is weakness
- slight fever
- loss of body weight.
- there may be tachycardia,
- pain in the liver.

Symptoms during an exacerbation
During the period of exacerbation, symptoms of intoxication appear:
- fever,
- weakness,
- malaise.
A distinctive feature of ulcerative colitis from simple catarrhal is weight loss. Patients often look emaciated. They have decreased appetite. With intestinal colitis, ulcerative defects are formed. When stool passes, they may bleed.
Symptoms may get weaker, then get worse again. With continued treatment, the remission phase sets in and the symptoms subside. How often relapses occur is determined by the treatment, and not by how much the intestine is affected.
Consequences and possible complications
In the absence of drug therapy and non-compliance with the diet, complications may develop. In this case, the symptoms of ulcerative colitis become more pronounced. The following consequences of colon inflammation are possible:
- massive bleeding;
- toxic expansion of the intestine (formation of a megacolon);
- perforation;
- malignancy of ulcers;
- inflammation of the joints;
- damage to internal organs (gallbladder, liver, skin).
Diagnostics
Ulcerative colitis is diagnosed and treated by a therapeutic specialist or gastroenterologist. Suspicion of a disease causes a set of corresponding symptoms:
- diarrhea mixed with blood, mucus and pus
- abdominal pain;
- arthritis disorders of the eyes against the background of general intoxication of the body.
Laboratory diagnostic methods:
- clinical blood test (increase in the number and ESR, decrease in the level of hemoglobin and erythrocytes);
- biochemical blood test (increased content of C-reactive protein and immunoglobulins);
- biopsy - histological examination of tissue samples;
- analysis of feces for fecal calprotectin - a special marker for the diagnosis of intestinal diseases, which in ulcerative colitis can increase to 100 - 150;
- coprogram (presence of occult blood, leukocytes and erythrocytes).
If the results of the tests carried out confirm the presence of a disease, the doctor prescribes an instrumental examination. An endoscopy is performed to detect possible edema on the mucous membrane, the presence of pseudopolyps, pus, mucus, blood in the intestine and to determine the extent of organ damage.
Endoscopic examinations (colonoscopy, rectosigmoidoscopy) reveal a complex of symptoms characteristic of pathology in a patient:
- the presence of mucus, blood, pus in the lumen of the intestine;
- contact bleeding;
- pseudopolyps;
- granular character, hyperemia and edema of the mucous membrane;
- in the phase of remission, atrophy of the intestinal mucosa is noted.
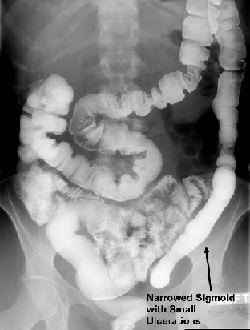
X-ray examination is also one of the effective methods for the diagnosis of ulcerative colitis. A barium mixture is used as a contrast agent in this procedure. On the roentgenogram of a patient with ulcerative colitis, enlargement in the lumen of the large intestine, shortening of the intestine, the presence of ulcers, polyps are clearly visualized.
Ulcerative colitis treatment
Treatment will be symptomatic, it should eliminate the process of inflammation and maintain remission, as well as prevent complications. If medications are not effective, surgery may be indicated.

The tasks of treating a patient with UC are:
- achieving and maintaining remission (clinical, endoscopic, histological),
- minimization of indications for surgical treatment,
- reducing the incidence of complications and side effects of drug therapy,
- reduction of hospitalization time and cost of treatment,
- improving the patient's quality of life.
The results of treatment largely depend not only on the efforts and qualifications of the doctor, but also on the willpower of the patient, who clearly follows the medical recommendations. The modern medicines available in the doctor's arsenal allow many patients to return to normal life.
Medications
To achieve these goals in reality, experts prescribe the following methods of treatment for patients with intestinal ulcerative colitis:
- taking non-steroidal anti-inflammatory drugs, for example, Salofalk, Dipentum, Sulfasalazine;
- the use of corticosteroids (metiprednisolone, prednisolone);
- antibiotic therapy by using drugs such as Tienam, Tsifran, Ciprofloxacin, Ceftriaxone;
- taking immunomodulators (Azathioprine, Cyclosporine, Infliximab, Methotrexate);
- the use of calcium and vitamins A, C, K.
In the case of the development of purulent complications or the addition of an infection, systemic antibacterial drugs are used. Medicines alone cannot cure a person. In the phase of remission in the absence of pain and bleeding, physiotherapy procedures are prescribed. The most frequently carried out:
- Exposure to alternating current.
- Diadynamic therapy.
- Interference therapy.
Patients with mild to moderate ulcerative colitis can be treated on an outpatient basis. Severe patients must be examined and treated in a hospital, since both diagnostic and therapeutic interventions can have serious and even life-threatening complications.
With the correct implementation of the doctor's recommendations, daily adherence to dietary prescriptions, as well as supportive therapy, it is possible to significantly increase the remission time and improve the patient's quality of life, but, unfortunately, full recovery cannot be achieved with the treatment of this disease.
Operation
Surgical treatment of ulcerative colitis is indicated for patients who are not helped by conservative methods. The indications for surgery are:
- perforation (perforation of the intestinal wall);
- signs of intestinal obstruction;
- abscess;
- the presence of a toxic megacolon;
- profuse bleeding;
- fistulas;
- bowel cancer.
To treat ulcerative intestinal colitis surgically today is possible in the following ways:
- by means of partial or total colectomy - excision of the colon;
- with the help of proctocolectomy - removal of the colon and rectum leaving the anus;
- by proctocolectomy and the imposition of a temporary or lifelong ileostomy, through which natural waste is excreted from the body.
It is necessary to pay attention to possible physical and emotional problems after surgery; care should be taken to ensure that the patient receives all necessary instructions before and after surgery and provide him with all possible medical and psychological support.
Knowing exactly what ulcerative colitis is and how to treat it, we can say with confidence that the prognosis of the disease is quite favorable. The pathological process is curable thanks to modern methods of therapy. Most patients are in complete remission, and only 10% of cases persist with unexpressed clinical symptoms.
Diet and nutrition

In this disease, the normalization of nutrition is of paramount importance. The diet for ulcerative colitis is aimed at mechanical, thermal and chemical sparing of the colon mucosa.
- The diet is based on the use of chopped, gentle food, steamed or boiled.
- Forever it is worth forgetting about hot sauces, fatty spices, alcohol, cigarettes.
- Fruits and vegetables should be consumed only in thermally processed form, because in their raw form they contain a lot of fiber, which negatively affects the functioning of the affected intestines.
- With an exacerbation, the diet includes liquid and pureed cereals (rice, semolina) in water (milk and broths are excluded). Buckwheat porridge enhances motor skills, therefore, during exacerbation, it is not recommended. It is convenient to use cereals for baby food, but they need to be diluted in half with water.
| Allowed Products: | With ulcerative colitis from the diet you need exclude the following foods and dishes: |
|
|
To find out exactly what products are allowed to eat for you, consult your doctor.
Ulcerative colitis menu for the day
Diet for ulcerative colitis of the intestine can be implemented through the following menu option.
- Breakfast: cereal porridge with 1 tsp. ghee, steam cutlet, rosehip decoction.
- Lunch: curd mass, berry jelly.
- Lunch: potato soup with meatballs, rice and minced meat casserole, compote.
- Afternoon snack: green tea, crackers.
- Dinner: stewed vegetables, fish cutlet, tea.
- Before bed: kefir / baked apple.
This menu option is suitable for the post-exacerbation period. Additionally, you can eat 200-250 grams of dried bread, 1 glass of jelly or compote.
Diet for ulcerative colitis of the colon, including rectum, leads to a number of positive changes:
- promotes the early restoration of normal stool, eliminating diarrhea or constipation;
- increases the effectiveness of medications, as it compensates for protein losses, accelerates the healing of the mucous membrane, due to which a number of medications begin to act more actively;
- compensates for the loss of nutrients, restores metabolism and energy reserves.
Folk remedies
In therapeutic therapy, it is allowed to use folk remedies, but only if the disease is at the initial stage of development and treatment is agreed with the doctor. The most effective methods of treating the disease, according to patients' reviews, are fasting, refusal to eat animal food, and a transition to a raw food diet. From herbal remedies, decoctions of yarrow, alder cones, wormwood, sage, and potato juice help well.
- 100 g in dried watermelon rind pour 2 cups of boiling water, insist and strain. Take up to 6 times a day for 100 g. This allows you to relieve inflammation in the intestines in acute and chronic forms of the disease.
- Perfectly relieves inflammatory processes in the intestines potato juice... It is enough to grate the potato, squeeze the juice out of it and drink it half an hour before meals.
- Take equal parts of the peppermint leaf, chamomile inflorescences, erect cinquefoil rhizomes. Insist 1 tablespoon of the mixture for 30 minutes in 1 cup of boiling water, drain. Take 1 glass 2-3 times a day for colitis.
- Treat flare-up symptoms bird cherry helps well... Traditional healers are recommended to prepare a decoction (one spoonful of flowers per glass of water). Take three times, every day for ¼ glass.
Prevention
Prevention of the development of this intestinal pathology consists in proper nutrition and periodic examination. It is important to treat chronic diseases of the digestive tract in a timely manner. The prognosis for ulcerative colitis in the absence of complications is favorable.
Ulcerative colitis is a serious disease that requires immediate and competent treatment. Do not postpone a visit to the doctor when the first symptoms appear. It is important to remember that in the event of an acute form of the disease, the organ is quickly affected, which can lead to the development of cancer or various complications.
- This is a diffuse ulcerative-inflammatory lesion of the mucous membrane of the large intestine, accompanied by the development of severe local and systemic complications. The clinic of the disease is characterized by cramping abdominal pain, diarrhea mixed with blood, intestinal bleeding, and extraintestinal manifestations. Ulcerative colitis is diagnosed based on the results of colonoscopy, irrigoscopy, CT, endoscopic biopsy. Treatment can be conservative (diet, physiotherapy, medication) and surgical (resection of the affected area of the colon).
General information
Ulcerative colitis (UC) is a type of chronic inflammatory disease of the large intestine of unknown etiology. It is characterized by a tendency to ulceration of the mucous membrane. Pathology proceeds cyclically, exacerbations are replaced by remissions. The most characteristic clinical signs are blood-streaked diarrhea, abdominal pain of a spastic nature. Long-term ulcerative colitis increases the risk of colon cancer.
The incidence is about 50-80 cases per 100 thousand population. At the same time, 3-15 new cases of the disease are detected annually for every 100 thousand inhabitants. Women are more prone to the development of this pathology than men, they have NUC 30% more often. Ulcerative colitis is characterized by primary detection in two age groups: young people (15-25 years old) and older people (55-65 years old). But besides this, the disease can occur at any other age. Unlike Crohn's disease, ulcerative colitis affects the mucous membrane of only the colon and rectum.

Causes
Currently, the etiology of ulcerative colitis is unknown. According to the assumptions of researchers in the field of modern proctology, immune and genetically determined factors may play a role in the pathogenesis of this disease. One of the theories of ulcerative colitis occurrence suggests that viruses or bacteria that activate the immune system, or autoimmune disorders (sensitization of immunity against one's own cells) may be the cause.
In addition, it was noted that ulcerative colitis is more common in people whose close relatives suffer from this disease. Currently, genes have also been identified that are likely to be responsible for a hereditary predisposition to ulcerative colitis.
Classification
Ulcerative colitis is distinguished by the localization and prevalence of the process. Left-sided colitis is characterized by lesions of the descending colon and sigmoid colon, proctitis is manifested by inflammation in the rectum, with total colitis, the entire large intestine is affected.
NUC symptoms
As a rule, the course of ulcerative colitis is wavy, periods of remission are replaced by exacerbations. At the time of exacerbation, ulcerative colitis manifests itself in various symptoms depending on the localization of the inflammatory process in the intestine and the intensity of the pathological process. With a predominant lesion of the rectum (ulcerative proctitis), bleeding from the anus, painful tenesmus, pain in the lower abdomen may occur.  Sometimes bleeding is the only clinical manifestation of proctitis.
Sometimes bleeding is the only clinical manifestation of proctitis.
With left-sided ulcerative colitis, when the descending colon is affected, diarrhea usually occurs, and the feces contain blood. Abdominal pain can be quite pronounced, cramping, mainly on the left side and (with sigmoiditis) in the left iliac region. Decreased appetite, prolonged diarrhea and indigestion often lead to weight loss.
Total colitis is manifested by intense abdominal pain, constant profuse diarrhea, severe bleeding. Total ulcerative colitis is a life-threatening condition, as it threatens the development of dehydration, collapse due to a significant drop in blood pressure, hemorrhagic and orthostatic shock.
The fulminant (fulminant) form of ulcerative colitis is especially dangerous, which is fraught with the development of severe complications up to rupture of the colon wall. One of the most common complications in this course of the disease is toxic enlargement of the large intestine (megacolon). It is assumed that the onset of this condition is associated with blockade of intestinal smooth muscle receptors by an excess of nitric oxide, which causes total relaxation of the muscle layer of the large intestine.
In 10-20% of cases, patients with nonspecific ulcerative colitis have extraintestinal manifestations: dermatological pathologies (pyoderma gangrenous, erythema nodosum), stomatitis, inflammatory eye diseases (iritis, iridocyclitis, uveitis, scleritis and episcleritis), joint diseases (arthritis, sacroiliitis, spondylitis) ), lesions of the biliary system (sclerosing cholangitis), osteomalacia (softening of the bones) and osteoporosis, vasculitis (vascular inflammation), myositis and glomerulonephritis.
Complications
A fairly common and serious complication of ulcerative colitis is toxic megacolon - expansion of the large intestine as a result of paralysis of the muscles of the intestinal wall in the affected area. With a toxic megacolon, intense pain and bloating in the abdomen, fever, and weakness are noted.
In addition, ulcerative colitis can be complicated by massive intestinal bleeding, intestinal rupture, narrowing of the colon lumen, dehydration as a result of large fluid loss with diarrhea, and colon cancer.
Diagnostics
The main diagnostic method that detects ulcerative colitis is colonoscopy, which allows you to examine in detail the lumen of the large intestine and its inner walls. Irrigoscopy and X-ray examination with barium allows you to detect ulcerative defects in the walls, changes in the size of the intestine (megacolon), violation of peristalsis, narrowing of the lumen. Computed tomography is an effective method of bowel imaging.
In addition, a coprogram, an occult blood test, and bacteriological culture are performed. A blood test for ulcerative colitis shows a picture of nonspecific inflammation. Biochemical indicators can signal the presence of concomitant pathologies, digestive disorders, functional disorders in the work of organs and systems. During a colonoscopy, a biopsy of the altered portion of the colon wall is usually taken for histological examination.
NUC treatment
 Since the causes of ulcerative colitis are not fully understood, the tasks of treating this disease are to reduce the intensity of the inflammatory process, subside clinical symptoms and prevent exacerbations and complications. With timely correct treatment and strict adherence to the recommendations of the proctologist, it is possible to achieve a stable remission and improve the patient's quality of life.
Since the causes of ulcerative colitis are not fully understood, the tasks of treating this disease are to reduce the intensity of the inflammatory process, subside clinical symptoms and prevent exacerbations and complications. With timely correct treatment and strict adherence to the recommendations of the proctologist, it is possible to achieve a stable remission and improve the patient's quality of life.
Ulcerative colitis is treated with therapeutic and surgical methods, depending on the course of the disease and the patient's condition. One of the important elements of symptomatic treatment of ulcerative colitis is dietary nutrition.
In severe cases of the disease in the midst of clinical manifestations, the proctologist may recommend a complete rejection of food intake, limiting the use of water. Most often, patients with an exacerbation lose their appetite and tolerate the ban quite easily. If necessary, parenteral nutrition is prescribed. Sometimes patients are transferred to parenteral nutrition in order to more quickly alleviate the condition with severe colitis. Food intake is resumed immediately after appetite is restored.
Diet recommendations for ulcerative colitis are aimed at stopping diarrhea and reducing irritation by food components of the intestinal mucosa. Products containing dietary fiber, fiber, spicy, sour foods, alcoholic beverages, and rough foods are removed from the diet. In addition, patients suffering from chronic intestinal inflammation are advised to increase the protein content in the diet (at the rate of 1.5-2 grams per kilogram of body per day).
Drug therapy for ulcerative colitis includes anti-inflammatory drugs, immunosuppressants (azathioprine, methotrexate, cyclosporine, mercaptopurine), and anticytokines (infliximab). In addition, symptomatic agents are prescribed: antidiarrheals, pain relievers, iron preparations with signs of anemia.
As anti-inflammatory drugs for this pathology, non-steroidal anti-inflammatory drugs are used - derivatives of 5-aminosalicylic acid (sulfasalazine, mesalazine) and corticosteroid hormonal drugs. Corticosteroid drugs are used during a period of severe exacerbation in the case of severe and moderate severity (or if 5-aminosalicylates are ineffective) and are not prescribed for more than a few months.
Children should be prescribed corticosteroid hormones with extreme caution. Anti-inflammatory hormone therapy can cause a number of severe side effects: arterial hypertension, glucosemia, osteoporosis, etc. From physiotherapeutic methods of treatment for ulcerative colitis, diadynamic therapy, SMT, interference therapy, etc. can be used.
Indications for surgical treatment are the ineffectiveness of diet and conservative therapy, the development of complications (massive bleeding, colon perforation, with suspicion of a malignant neoplasm, etc.). Resection of the large intestine followed by the creation of an ileorectal anastomosis (the connection of the free end of the ileum with the anal canal) is the most common surgical technique for the treatment of ulcerative colitis. In some cases, an area of the affected intestine that is limited within healthy tissues is removed (segmental resection).
Forecast and prevention
There is currently no prophylaxis for ulcerative colitis, since the causes of this disease are not fully understood. Preventive measures for the occurrence of relapses of exacerbation are compliance with the doctor's instructions for lifestyle (nutritional recommendations similar to those in Crohn's disease, reducing the number of stressful situations and physical overstrain, psychotherapy) and regular dispensary observation. A good effect in terms of stabilizing the condition is provided by spa treatment.
With a mild course without complications, the prognosis is favorable. About 80% of patients taking 5-acetylsalicylates as maintenance therapy do not notice relapses and complications of the disease throughout the year. In patients, relapses usually occur 1 time in five years, in 4% of exacerbations are absent within 15 years. Surgical treatment is used in 20% of cases. The likelihood of developing a malignant tumor in patients with NUC ranges from 3-10% of cases.
Medical treatment for ulcerative colitis
MD, prof. V.G. Rumyantsev, Head of the Department of Colon Pathology, Central Research Institute of Gastroenterology, Moscow Department of Health
Ulcerative colitis is a disease of unknown etiology with a chronic, undulating course. Its morphological basis is a superficial, diffuse inflammation of the mucous membrane, initiated in the rectum and spreading in the proximal direction. The process does not go beyond the colon and therefore the patient can be relieved of painful sensations by radical surgical intervention. Drug therapy allows you to control the course of the disease with an acceptable level of quality of life. It is encouraging that the course of even total colitis is becoming more favorable. The severity of attacks and the frequency of exacerbations are reduced, often the process regresses, limited to the rectum and sigmoid colon. Thus, nonsurgical treatment remains the leading treatment for ulcerative colitis. The superficial nature of inflammation and the obligatory involvement of the rectum predetermines three essential features of the treatment of the disease: first, the effectiveness of "locally" acting anti-inflammatory drugs, in particular sulfasalazine and its analogs; second - the need to use rectal dosage forms; and, finally, third - less successful than in Crohn's disease, the effect of immunomodulatory agents. The choice of therapy is based on the localization and extent of the lesion, the severity of the attack, sensitivity and refractoriness to certain drugs, the fundamental possibility of achieving remission in this patient.
Purpose of therapy
It is extremely important for the clinician to clearly understand the purpose of therapy of the disease, taking into account the real possibilities of drug treatment. Remains a controversial issue regarding the possibility of achieving "biological" remission. So, with ulcerative colitis, asymptomatic patients in 35-60% of cases retain endoscopic activity, and 90% of patients, even with endoscopic remission, show histological signs of inflammation, of which a third is acute.
Endoscopic and histological remission is delayed. When should therapy be discontinued? The answer to this question is given by a retrospective analysis of the frequency of exacerbations. If with endoscopic remission during the year 4% of exacerbations of ulcerative colitis are observed, then with persisting endoscopic activity - already 30%. The presence of histological signs of acute inflammation increases the risk of exacerbations by another 2-3 times. Therefore, in all cases of recurrent ulcerative colitis, one should strive for histological remission, which is the basis for stopping therapy. This rule does not apply to chronically continuous or active type of the course of the disease, severe acute form, patients with frequent exacerbations. In these cases, long-term supportive therapy and a change in landmarks may be required - to achieve a minimum level of activity at which the patient is relieved of painful symptoms and maintains a normal quality of life, to avoid surgery or frequent repeated exacerbations. From a practical point of view, it is important that the induction of clinical endoscopic remission should be the goal of treating any newly diagnosed ulcerative colitis, chronically recurrent forms of the disease and those chronically active cases where therapy is recognized as inadequate. If endoscopic control is impossible, the following rule should be used: therapy is carried out until the stool is normalized and then for at least 3 weeks, which should be sufficient to achieve an endoscopic effect.
Mild to moderate attack of distal colitis
Distal ulcerative colitis is a concept that includes three main forms of the disease: proctitis - an inflammatory process up to 20 cm from the edge of the anus, proctosigmoiditis (from 20 to 40 cm) and left-sided colitis (40-80 cm). They make up 60-70% of all cases of ulcerative colitis in total, have important features of pathogenesis, clinical picture and treatment that distinguish them from total lesions of the colon. These differences are due to the unequal functional activity of the right and left half of the colon, the peculiarities of motility, absorption and metabolism in the intestinal wall. Distal colitis occurs without systemic complications. As a result of the delay in intestinal contents above the zone of active inflammation, false desires with mucus and blood often come to the fore in the clinical picture, with constant "trauma" of the mucous membrane with densely formed feces. Urgent urge may be accompanied by anal incontinence. The availability of the inflammation zone for rectally administered drugs, the high concentration they create in the intestinal wall and low concentration in the systemic circulation serve as a prerequisite for predominantly local therapy of distal ulcerative colitis. The clinical effect with rectal administration of drugs is almost always higher than with oral administration. By manipulating the volume and rate of administration, using different dosage forms, it is possible to ensure the delivery of the drug to the desired segment of the colon. The liquid enema reaches the splenic flexure, and with a volume of more than 100 ml, it moves further in the proximal direction. Foam is distributed in the rectum and sigmoid colon, and suppositories are limited only to the rectum.
Many drugs have been proposed for the local treatment of ulcerative colitis, but only corticosteroids acting on the "proximal" mediators of the immune-inflammatory cascade and aminosalicylates, which also act on multiple, but "distal" links of pathogenesis, are recognized as the basic ones. The use of liquid enemas of glucocorticoids was first proposed in the 1950s, and their proven ability to reduce the inflammatory response on contact with the mucosa made this therapy popular. Rectally administered steroids are poorly absorbed and therefore safer than oral steroids. Short courses of rectally administered corticosteroids (prednisolone at a dose of 20-40 mg / day, hydrocortisone - 100-250 mg / day, etc.) are effective in the treatment of distal ulcerative colitis of any severity, but it is not recommended to use them continuously to maintain remission due to side effects. phenomena. And this small risk is enough to strive to use "systemic" glucocorticoids for strict indications. An alternative in the treatment of distal colitis is the use of 5-aminosalicylic acid (5-ASA) or topical steroids. 5-ASA drugs are as effective in treating active inflammation as glucocorticoids, and even surpass them. They also help those patients in whom hydrocortisone therapy was unsuccessful. It should be noted that the effective dose of rectally administered 5-ASA drugs can vary widely - from 1 to 4 g per day. In a double-blind controlled study in 287 patients, the effect of placebo was compared, as well as 5-ASA at a dose of 1, 2 and 4 g / 10 /. Clinical improvement against the background of placebo was obtained in 27% of patients, against the background of 5-ASA - in 67, 65 and 75%, respectively. The drug was safe not only in traditional amounts, but also when administered intraintestinal at a dose of 8 g / day. Aminosalicylates in Europe and the United States are considered first-line drugs for ulcerative colitis, while glucocorticoids are used in the absence of an effect or allergy to 5-ASA. Before prescribing systemic steroids, budesonide is used in enemas at 2 mg / day. The drug has a high affinity for hormonal receptors and 90% of it is converted into metabolites devoid of biological activity already during the first passage through the liver. Budesonide enemas were comparable in induction of remission with systemic hormones, but weaker than 5-ASA at a dose of 4 g. The drug did not inhibit the pituitary-adrenal axis, and in combination with mesalazine provided an effect that exceeded the effect of each drug separately. The possibility of inducing remission of distal colitis using monotherapy with sulfasalazine and its analogues is excluded, although such attempts are still often made. This is due to the fact that oral drugs do not create a therapeutic concentration in the mucous membrane of the rectum and sigmoid colon. 5-ASA is released in the right colon, and only a small amount reaches the rectum. The study of the concentration of the drug in the intestinal mucosa shows that only rectal administration can count on the effect. Both systemic steroids and 5-ASA can be used to induce remission of distal colitis. All other things being equal, you need to use the drug to which the patient's sensitivity is higher and change it when resistance is detected. Usually the effect is manifested
after 1-2 weeks, but the treatment of active distal colitis is continued for the period necessary to achieve complete clinical and endoscopic remission - 6-8 weeks. With a prolonged attack, prolonged treatment is justified with a transition to intermittent administration of drugs 2-3 times a week. If treatment with rectal 5-ASA drugs does not lead to the desired result, therapy can be enhanced by a combination with topical steroids or additional oral administration of 5-ASA. Oral drugs are always prescribed for left-sided colitis and can be used for more limited lesions in order to prevent the progression of the process in the proximal direction.
Common mild to moderate ulcerative colitis
In the treatment of mild to moderate colitis, sulfasalazine and its analogues are used orally in combination with local therapy. Which 5-ASA drugs should I give preference to? If sulfasalazine is well tolerated, there is no need to use “pure” 5-ASA preparations. Side effects of sulfasalazine (headache, nausea, vomiting, dizziness) are caused by toxic concentrations of sulfapyridine due to its slow or weak acetylation in the liver.
Slow acetylators suffer earlier and more severely. Special studies have found that in the United States, up to 60% of people in the general population belong to slow acetylators, while in Japan up to 90% are fast ones. As for Russia, there is no information about this. It can be assumed that the genetically determined "slow" type of acetylation is less common than in the United States and Europe. Sulfasalazine is used in the active phase of the disease at a dose of 4-6 g per day. In case of toxic reactions, the search for a tolerable dosage begins with 0.5 g, gradually increasing over several weeks to 2 g / day ("titration" method). For those patients who develop an allergy in the form of a rash and fever, you can start taking sulfasalazine with a dose of 1 mg, slowly increasing it over 2-3 months. In recent years, these techniques have been rarely used due to the degree of risk and the existence of safe alternative therapies. These include preparations of "pure" 5-ASA (Mesacol, Salofalk, Pentasa). They lack sulfapyridine and the release of 5-ASA is based on pH and time-dependent mechanisms. Mesacol releases 5-ASA in the colon at pH-7, Salofalk - in the terminal ileum at pH-6, Pentasa - throughout the small intestine. They are equally useful in the treatment of advanced ulcerative colitis, although more distal-release drugs appear to be preferable. In contrast to the topical application of 5-ASA, where the dose-dependent effect of the drug has not been established, oral aminosalicylates act the more efficiently, the higher the dose. Sutherland et al. / 32 / conducted a meta-analysis of 8 trials involving 1000 patients, which compared 5-ASA and placebo in the induction of remission of ulcerative colitis. The dose-dependent effect was confirmed: a) less than 2.0 g per day, OR - 1.5; 95%; CI 0.89-2.6; b) from 2.0 to 2.9 g / day, OR - 1.9; 95%; CI 1.3-2.8; c) more than 3.0 g per day, OR - 2.7; 95%; CI 1.8-3.9. At least 80% of patients with moderate ulcerative colitis can respond to 5-ASA therapy at a dose of 2.0-4.8 g / day. Research is ongoing to establish safe upper dose limits for 5-ASA ..
As already indicated, in the treatment of advanced ulcerative colitis, it is imperative to combine oral and rectal dosage forms. Aminosalicylate therapy for advanced colitis can be flexible. Therapy is usually started with sulfasalazine. There are two reasons for switching a patient to "pure" 5-ASA drugs - serious side effects and the need for high doses. If sulfasalazine is ineffective, 5-ASA preparations with pH-dependent release are used. If the capsules are excreted unchanged in the faeces, then this serves as a signal for the use of 5-ASA with time-dependent coating.
Treatment for severe ulcerative colitis
In the treatment of severe attack of ulcerative colitis, there is no alternative to corticosteroids. Usually, preference is given to parenteral use of hydrocortisone 400 mg / day or prednisolone 120 mg / day for 5-7 days, after which the patient is transferred to oral administration at the rate of 1.0-1.5 mg / kg of body weight. Treatment continues for 3 or more months, gradually reducing the dose. The remission rate is approaching 80%. With a moderate attack of ulcerative colitis, therapy is immediately started with prednisolone tablets. The initial dose differs from center to center. There are at least three approaches to dose selection: the first is the minimum dose with a gradual increase to the optimal dose, the second is the average dose sufficient for the vast majority of patients and, finally, a deliberately excessive dose, which is corrected after the clinical effect is achieved, taking into account its speed. offensive. However, in our opinion, the first admission is unacceptable in cases of severe colitis, since it takes a long time to find an effective dose, and this is fraught with the development of complications and unjustified surgical intervention. Decrease of the "oversized" dose may be slow or
fast. Starting at a dose of 30 mg / day, aminosalicylates are added, which are left as maintenance treatment after corticosteroid withdrawal. In order to prevent osteoporosis, patients are prescribed calcium and vitamin D preparations.
The concomitant use of oral aminosalicylates with steroids in severe ulcerative colitis is not supported for the following reasons:
1) they are weaker than glucocorticoids in terms of anti-inflammatory effect;
2) aminosalicylates reduce the response to steroids;
3) side effects that occur when taking aminosalicylates can worsen the course of colitis, and therefore simulate resistance.
There is no consensus regarding pulse therapy and short courses of hormonal therapy. Perhaps the successful use of pulse therapy with methylprednisolone at a dose of 1 g / day or dexamethasone at a dose of 100 mg / day in the form of 3-day infusions. However, short courses of hormonal therapy in order to interrupt the attack are effective only during the period when the first signs of an exacerbation appear in severe patients with inflammatory bowel diseases. In this case, therapy with high doses of steroids is continued for no more than 10-14 days, with the transition to intermittent hormones or aminosalicylates. This is the period during which hormonal treatment can be stopped without "withdrawal syndrome". Of course, this is possible only in young patients in the absence of serious concomitant diseases and previous long-term hormonal therapy.
The continuous course of ulcerative colitis and hormonal dependence
There is a category of patients in whom, even in conditions of adequate treatment, it is not possible to achieve sustained improvement or remission, requiring constant maintenance therapy. These can be patients with distal or advanced colitis with varying degrees of activity. Among them are patients with hormonal dependence. Hormonal dependence is considered to be the impossibility to reduce the dose of prednisolone below 10 mg / day without exacerbation of the disease or an outbreak of the process within 3 months after the termination of hormonal treatment / 7 /. In this case, there are four possibilities: the use of sparing intermittent hormone intake, transfer to topical steroids, the use of azathioprine / methotrexate or infliximab. Intermittent hormone intake has been borrowed from pediatric practice.
It has been shown that the optimal dose is to take 40 mg of prednisolone every other day. The best results and minimal side effects were observed at this dose. No suppression of the pituitary adrenal axis was observed, which made it possible to discontinue treatment at once, without fear of "withdrawal syndrome". This scheme has been successful in patients with frequent exacerbations and chronic continuous disease. Two methods of transition from the basic course of hormonal therapy have been developed: by transferring 1 tablet (5 mg) of prednisolone from one day to another every 10 days, or by reducing the dose by 5 mg on every second day with an interval of 6-10 days. The first method was more reliable and gave reactivation less often.
Transfer of the patient to topical steroids (budesonide) can also avoid dangerous side effects. Literature data indicate that in 2/3 of hormone-dependent patients it is possible to reduce or cancel systemic steroids. It must be remembered that the recommended dose of budesonide (9 mg / day) corresponds to 30 mg of prednisolone. They are prescribed simultaneously and only then gradually reduce systemic steroids until complete cancellation.
Much more often in the treatment of hormone-dependent forms of inflammatory bowel diseases, immunosuppressants, in particular azathioprine, are used. Analysis of more than 20-year experience of its use in hormone-dependent ulcerative colitis showed that induction of remission with simultaneous withdrawal of steroids becomes possible in 40-80% of patients. Azathioprine therapy is continued for 4 years or more. However, it should be borne in mind that the action of the drug is delayed and appears no earlier than 3 months. Therefore, it is important to use an adequate dose of azathioprine (2.0-2.5 mg / kg) and duration (at least 6 months). The drug is relatively safe, but individuals with genetically low thiopurine methyltransferase activity may develop leukopenia and sepsis. Treatment with azathioprine is contraindicated in them. Fortunately, monozygous low thiopurine methyltransferase activity is rare - only 0.3% of cases. Another 11.1% have heterozygous or intermediate activity, requiring a dose reduction by 50%.
If the effect is insufficient, they resort to the appointment of methotrexate. It is an analogue of dehydrofolic acid, which exhibits immunomodulatory properties in low doses.
Methotrexate at a dose of 25 mg per week IM or SC has been shown to be effective in inducing and maintaining remission of Crohn's disease. However, it can be successfully applied in a number of cases of ulcerative colitis. The side effects are relatively minor. Limit the use of methotrexate teratogenic effect, hepatotoxicity and the possibility of developing liver fibrosis with prolonged use. The drug can also be used orally in the form of 5 mg tablets every other day, but the bioavailability of oral methotrexate varies significantly. This method of administration is suitable only during the period of maintenance of remission.
Infliximab has been used in recent years when treatment has failed, is intolerant to these immunosuppressive drugs, or a rapid response is required. The introduction of intravenous infliximab at a dose of 5 mg / kg allows to stop active manifestations of the disease, and repeated infusions every 8 weeks - to maintain remission. Infliximab has a sparring effect on glucocorticoids. It is recommended for use throughout the year as monotherapy or in combination with azathioprine.
Hormonal resistance
Hormonal resistance is the most serious problem clinicians face. The definition of "resistance" is especially difficult in adrenal colitis. So, in a severe attack, resistance is established after the first 5 days of intensive hormonal therapy, and in distal forms - after 6-8 weeks of treatment - 5-ASA inside and topically - with steroids. There is much that is unclear in the appearance of hormonal resistance. Some describe a reduced level of receptors only in resistant patients, others - in all, without exception, in comparison with controls. Corticosteroid receptors express either an active alpha chain or its opposite, beta. The latter is determined precisely with hormonal stability / 1 /. Patients with ulcerative colitis with a high level of antineutrophilic cytoplasmic antibodies show refractoriness. In addition, in this process, the increased expression of the multidrug resistance gene detected in the peripheral lymphocytes of patients with inflammatory diseases of the colon in need of surgery may be important / 8 /.
For ulcerative colitis, cyclosporine is prescribed after 5 days of unsuccessful IV corticosteroid therapy. It is a potent immunosuppressant with a selective effect on the T-lymphocytic immune response, inhibiting the transcription and formation of IL-2 and interferon-gamma. The increasing use of cyclosporine in clinical practice confirms the usefulness of this treatment. Colectomy is usually avoided in 40-69% of patients. The protocol for the use of cyclosporine provides for starting treatment with an intravenous infusion at a dose of 2-4 mg / kg and maintaining a blood concentration of no more than 500 ng / ml for 7-10 days. Then the patient is transferred to taking the drug orally at a dose of 5-8 mg / kg and the concentration is controlled at about 300 ng / ml. Later, it was shown that a similar effect can be obtained with oral microemulsion cyclosporin at a dose of 5 mg / kg with high bioavailability. Treatment is continued for 3 months, combined with the appointment of azathioprine, which is left as maintenance therapy. Usually, they fear well-established side effects of cyclosporine (impaired renal function, hypertension) and control blood pressure, kidney and liver function, and monitor the concentration in the blood. Our experience of using neoral confirms the ability of cyclosporin to overcome hormonal resistance with a good long-term effect in 64% of patients. The concentration of cyclosporine in the blood varied from 80 to 170 ng / ml and in no case was treatment interrupted due to dangerous side effects. In our opinion, oral cyclosporine is a fairly safe and effective drug in the treatment of severe forms of ulcerative colitis, which can be used in wide clinical practice as an alternative to surgery.
For resistant forms of Crohn's disease, a new agent is used - infliximab. These are chimeric monoclonal antibodies to tumor necrosis factor. Its main mechanism of action is associated with the neutralization of this pro-inflammatory cytokine on cell membranes and the induction of apoptosis of activated T cells. The first experience of using infliximab in patients with ulcerative colitis did not allow making a final conclusion about the effectiveness of the drug in achieving remission of the disease, overcoming hormonal dependence and resistance. However, two published large randomized trials tipped the scales in favor of infliximab / 24, 29 /. In these studies, 364 patients who did not respond to at least one of the standard treatments (including oral 5-ASA) received infliximab at doses of 5 mg / kg, 10 mg / kg, or placebo. After a triple induction regimen at 0, 2, and 6 weeks, they received repeated infusions every 8 weeks. Not only clinical, but also endoscopic remission was achieved in 60-62% of patients taking infliximab at a dose of 5 mg / kg after 8 weeks. compared with 31-34% with placebo (P0.001). Moreover, remission was maintained at 54 weeks (46 versus 18%). Taken together, the results of these two studies clearly support the treatment of active refractory ulcerative colitis.
Although these data concern outpatients, it can be assumed that the drug is effective even with unsuccessful treatment with intravenous steroids / 12 /. Treatment with chimeric antibodies inevitably leads to the formation of antibodies to the drug itself, which is accompanied by an increased risk of infusion reactions and a decrease in the duration of response to therapy due to a decrease in the therapeutic concentration. The risk of antibody formation can be reduced by combination with other immunosuppressants, prior glucocorticoid administration, and regular supportive treatment. The risk of opportunistic infections and tuberculosis must be considered. A positive Mantoux reaction, even in the absence of X-ray changes in the lungs, is the basis for anti-tuberculosis therapy for at least a month, ahead of the infliximab infusion during this period.
Therapy should be carried out under supervision and control in a specialized medical institution equipped with the necessary equipment for intensive care of possible severe infusion reactions. The drug should not be used as a preliminary therapy for a refractory disease that is subject to surgical treatment. Although most experts believe that infliximab does not increase the risk of surgical complications, half of them still prefer to postpone surgery for 1 month after attempting drug treatment.
Infliximab treatment is safe during pregnancy and breastfeeding. It is contraindicated in active tuberculosis and other infections, in patients with heart failure, in demyelinating diseases, optic neuritis, in patients with a history of malignant neoplasms and lymphoma.
Maintaining remission
Ultimately, it is important not only to achieve remission, but also to maintain it as long as possible. For this purpose, I use primarily aminosalicylates. The optimal dose for maintenance treatment is 2 g / day, with which "addiction" does not develop and the protective effect lasts for many years. A meta-analysis comparing sulfasalazine and "new" aminosalicylates showed a slight advantage of sulfasalazine in maintaining remission of ulcerative colitis (OR - 1.29; 95%; CI - 1.06-1.57) / 33 /. According to the meta-analysis, a dose-dependent effect in maintaining remission is not observed, although a number of researchers believe that the maintenance dose should be equal to the dose of remission induction / 11 /. Apparently, in order to prevent exacerbation, both continuous and intermittent reception of 5 # ASA can be used. Mesalazine at a dose of 2.4 g / day for a week of each month was as effective as a continuous dose of 1.6 g / day, and the use of 3 g of sulfasalazine at the first symptoms of an outbreak led to the same result as regular reception 2 g / day. In order to maintain remission of distal colitis, both oral and rectal preparations in the form of suppositories and enemas can be equally used, and for an unlimited time / 4 /. With equal dosage, a single administration has advantages over multiple administrations. The unpopularity of rectal forms in patients can be tried to mitigate also by intermittent administration. It must be remembered that rectal treatment with 5-ASA for left-sided
colitis is better than placebo and oral mesalazine preparations (OR - 2.41; 95%; CI - 1.05-5.54) / 19 /, better than glucocorticoids (OR - 2.03; 95%; CI - 1.28-3 , 20) / 20 /, but inferior to the combined treatment (oral + local) / 6, 25 /. After suffering a severe attack of ulcerative colitis, maintenance treatment should be carried out for a long time - up to two years. If exacerbations are seasonal, then preventive therapy is usually sufficient only in the months of increased risk. If the treatment of 5-ASA is ineffective, they resort to taking azathioprine for 2-4 years. In recent years, interest in the use of probiotics as a means of preventing exacerbations of ulcerative colitis has increased significantly. As shown in two controlled studies, where patients with ulcerative colitis received 5-ASA or E. coli Nissle 1917 capsules as maintenance treatment, the effectiveness of probiotics and 5-ASA was the same / 15, 23 /.
Alternative treatment for ulcerative colitis
Many drugs have been proposed for the general and topical treatment of ulcerative colitis, although not all have been adequately tested in multicenter controlled clinical trials. As a rule, we are talking about ancillary or "adjuvant" therapy. This includes leukotriene B4 inhibitors, anesthetics, mast cell stabilizers, immunoglobulins, reparants, protectors, antioxidants and nicotine. Omega-3 polyunsaturated fatty acids (Eikanol) synergize with 5-ASA and corticosteroids by inhibiting leukotriene B4. The use of Eikanol or other fish oil preparations can be useful in the control of active ulcerative colitis or in the prevention of exacerbations / 17 /. For nonsmokers, nicotine is effective, applied in the form of applications on the skin at a dose of 5-22 mg or enemas at a dose of 6 mg.
The effect is moderate, 25-30% higher than placebo / 28 /. Topical sodium cromoglycate can be used as a trial treatment, especially if high levels of eosinophils are found in biopsies. The use of a mixture of short-chain fatty acids (butyric, acetic, propionic), which are essential elements for nutrition and regeneration of the colonic epithelium, aroused considerable interest. In a large controlled trial of short-chain fatty acids in enemas in 91 patients with left-sided ulcerative colitis, a positive effect was obtained in 65% of cases / 3 /. However, to date, it has not been possible to obtain pharmacologically stable drugs, and therefore the method is more often used in which prebiotics are administered, which enhance the endogenous synthesis of these acids. Thus, in 105 patients with ulcerative colitis, 5-ASA or Plantago ovata (Mukofalk) was used to maintain remission. The effect was the same, but after taking Mucofalk there was a significant increase in the content of butyric acid in feces / 9 /.
Other sources of dietary fiber, such as sprouted barley, can also be used to increase butyrate synthesis. In a controlled study in the active phase of ulcerative colitis and in the period of remission, it was shown that barley food significantly reduced the activity of the inflammatory process, allowed to reduce the intake of steroids and the frequency of exacerbations / 13 /. In the case when it is necessary to improve the retention function with active distal colitis, anesthetics are used - lidocaine or ropivacaine in a gel. It is curious that these drugs also significantly reduce the activity of inflammation, affecting its neurogenic component / 26 /. Substance P, which acts on neurokinin receptors, is known to be a mediator of neurogenic inflammation in the colon. In a pilot study of the neurokinin-1 receptor antagonist in ulcerative colitis, a more rapid disappearance of pain and bleeding was noted; by the end of 4 weeks, 5 out of 9 patients achieved remission / 35 /. In uncontrolled trials, the effect was also observed from intravenous transfusions of immunoglobulins (2 g / kg for 2-5 days, then 200-700 mg / kg every 2 weeks for 3-6 months) / 16 /. For some reason, arsenic preparations are rarely mentioned in the list of treatments for ulcerative colitis, although there have been quite encouraging results. Clinical experience shows that vaginal suppositories "Osarbon" can be successfully used with minimal activity of ulcerative colitis instead of traditional therapy. It is sometimes used as a topical treatment for an enema of sucralfate and bismuth subsalicylate. A number of studies have confirmed their effectiveness / 36 /.
If azathioprine is intolerant, it is recommended to replace it with mycophenolate mofetil, an immunosuppressive drug used in transplantology and in autoimmune disorders, where it turned out to be more effective than azathioprine / 31 /. It has already been tested in Crohn's disease, but it has been used relatively infrequently in ulcerative colitis. There is only one cohort study comparing mycophenolate mofetil 20 mg / kg / day with azathioprine in active ulcerative colitis. After 12 months, 88% of patients were in remission on this drug and 100% on azathioprine / 21 /.
The same replacement exists for cyclosporine - tacrolimus (FK-506), a macrolide immunosuppressant. There is a positive experience in the treatment of inflammatory bowel diseases. In the treatment of ulcerative colitis, a number of researchers include heparin with a low molecular weight, although the results of treatment are rather controversial / 2,
14, 18/.
Much effort is being made to find the optimal therapy for severe refractory colitis. These are anti-cytokine strategy and sorption methods. The use of leukocytopheresis in severe hormone-dependent ulcerative colitis is very successful. Compared with placebo, the effect was 80% versus 33% / 30 /, while the rate of clinical improvement increased in proportion to the rate of apheresis. So, when it is performed once a week, remission was achieved in 22.5 days, and when apheresis 2-3 times a week - in 7.5 days / 27 /. In the treatment of ulcerative colitis, pegylated interferon-alpha at a dose of 0.5 μg / kg can also be used. When using weekly injections for 12 weeks. clinical and endoscopic remission is achieved in 60% of patients / 34 /. The first trials of human monoclonal antibodies to CD3 lymphocytes / 22 /, antagonists of the IL-2 receptor / 5 /, look promising. Blocking chimeric monoclonal antibodies to CD25 have been shown to increase sensitivity to glucocorticoids, and therefore overcome hormonal resistance.
Thus, the arsenal of drugs suitable for use in the treatment of ulcerative colitis is constantly growing. Skillful use of unconventional techniques can increase the effectiveness of basic therapy, but enthusiasm for them to the detriment of proven and included in the standards of drugs would be a serious mistake, fraught with negative consequences for the patient. Knowledge of standards is essential because facilitates the doctor's choice of drugs, modes of their administration, guarantees the safety and high quality of medical care for these patients.
Literature
1. Ayabe T., Imai S., Ashida T. et al. Glucocorticoid receptor beta expression as a novel predictor for therapeutic efficacy of corticosteroid in patients with ulcerative colitis // Gastroenterology. 1998.114. A 924.
2. Bloom S., Kiilerich S., Lassen M.R. et al. Randomized trial of Tinzaperin, a low molecular weight heparin (LMWH) versus placebo in the treatment of mild to moderately active ulcerative colitis.// Gastroenterology. 2003.124.4. Suppl. 1.P. 540.
3. Breuer R.I., Soergel K.H., Lashner B.A. et al. Short chain fatty acid rectal irrigation for left-sided ulcerative colitis: A randomized, placebo controlled trial // Gut. 1997.40. P. 485-491.
4. Casellas F., Vaquero E., Armengol J.R., Malagelada J.R. Practically of 5-aminosalicylic suppositories for long-term treatment of inactive distal ulcerative colitis // Hepato-Gastroenterology. 1999 46 28 28 P. 2343-2346.
5. Creed T., Hearing S., Probert Ch. et al. Basiliximab (IL-2 Receptor antagonist) as a steroid sensitizing agent in steroid resistant ulcerative colitis // Gastroenterology. 2003 124 4. Suppl. 1.P. 65.
6. D'Albasio G., Pacini F., Camarri E. et al. Combined therapy with 5 # aminosalicylic acid tablets and enemas for maintaining remission in ulcerative proctitis: a randomized doubleblind study.// Am. J. Gastroenterol. 1997 92. P. 1143-1147.
7. ECCO Consensus on the Management of Crohn's disease. // Gut. 2006. 55 (Suppl. 1).
8. Farrel R. J., Murphy A., Long A. et al. High multidrug resistance (P-glycoprotein 170) expression in inflammatory bowel disease patients who fail medical therapy.// Gastroenterology. 2000. 118. P. 279-288.
9. Fernandez-Banares F., Hinojosa J., Sanches-Lombrana J.L. et al. Randomized clinical trial of Plantago ovata seeds (dietary fiber) as compared with mesalamine in maintaining remission in ulcerative colitis.// Am. J. Gastroenterol. 1999. 94. P. 427-433.
10. Hanauer S.B. Dose-ranging study of mesalamine (pentasa) enemas in the treatment of acute ulcerative proctosygmoiditis: Results of a multicentered placebo-controlled trial // Inflam. Bowel Dis. 1998. 4. P.79-83.
11. Hanauer S.B., Meyers S., Sachar D.B. The pharmacology of anti-inflammatory drugs in inflammatory bowel disease. In: Kirsner J.B., Shorter R.G., ed. Inflammatory bowel disease. 4 th ed. Baltimore. Williams and Wilkins. 1995. P. 643-663.
12. Jarnerot G., Hertervig E., Friis Liby I. et al. Inflixomab as rescue therapy in severe to moderately severe ulcerative colitis: a randomized, placebo-controlled study // Gastroenterology. 2005.128. P. 1805-1811.
13. Kanauchi O., Mitsnyama K., Andoh A. et al. Beneficial effects of prebiotics, germinated barley foodstuff, in the long term treatment of ulcerative colitis: a multicenter open control study // Gastroenterology. 2003. 124. 4. Suppl. 1.P. 1749.
14. Korzenik J., Miner P., Stanton D. et al. Multicenter, randomized, double-blind, lacebo-controlled trial of Deligoparin (ultra low molecular weight heparin) for active ulcerative colitis // Gastroenterology. 2003 124 124 4. Suppl. 1.P. 539.
15. Kruis W., Schutz E., Fric P. et al. Double-blind comparison of an oral Echerichia coli reparation and mesalazine in maintaining remission of ulcerative colitis.// Aliment. Pharmacol. Ther. 1997.15 P. 853-858.
16. Levine D.S., Fischer S.H., Christie G.L. et al. Intravenous immunoglobulin therapy for active, extensive, and medically refractory idiopathic ulcerative colitis and Crohn's disease.// Am. J. Gastroenterol. 1992. 87. P. 91-100.
17. Loeschke K., Ucberschaer B., Pietsch A. et al. N # 3 fatty acids retard early relapse in ulcerative colitis.// Abstract. Book AGA. 1996. A 781.
18. Marc A., De Bievre, Anton A. et al. A randomized, placebo-controlled trial of low molecular weight heparin in active ulcerative colitis.// Gastroenterology. 2003. 124. 4. Suppl. 1.P. 543.
19. Marshall J.K., Irvine E.J. Rectal aminosalicylate therapy for distal ulcerative colitis: a meta-analysis.// Aliment. Pharmacol. Ther. 1995.9.293-300.
20. Marshall J.K., Irvine E.J. Rectal corticosteroids vs. alternative treatment in ulcerative colitis: a meta-analysis.//Gut. 1997. 40. P. 775-781.
21. Orth T., Reters M., Schlaak J.F. et al. Mycophenolate mofetil versus azathioprine in patients with chronic active ulcerative colitis: a 12 # month pilot study // Am. J. Gastroenterol. 2000. 95. P. 1201-1207.
22. Plevy S. E., Salzberg B. A., Regueiro M. et al. A humanized anti-CD3 monoclonal antibody, Visilizumab, for treatment of severe steroid-refractory ulcerative colitis: Preliminary results of a phase 1 study // Gastroenterology. 2003. 124. 4. Suppl. 1.P. 62.
23. Rembacken B.J., Snelling A.M., Hawkey P.M. et al. Non-pathogenic Escherichia coli versus mesalazine for the treatment of ulcerative colitis: a randomized trial.// Lancet. 1999.21. P. 635-639.
24. Rutgeerts P., Feagan B., Olson A. et al. A randomized placebo-controlled trial of infliximab therapy for ulcerative colitis: Act 1 trial.// Gastroenterology. 2005.128.A 689.
25. Safdi M., DeMicco M., Sninsky C. et al. A double blind comparison of oral vs. rectal mesalamine vs. combination therapy in the treatment of distal ulcerative colitis // Am. J. Gastroenterol. 1997. 92. P. 1867-1871.
26. Saibil F.G. Lidocaine enemas for intractable distal ulcerative colitis: efficacy and safety // Gastroenterology. 1998. 114. Pt 2. P. 4395.
27. Sakuraba A., Naganuma M., Hibi T., Ishii H. Intensive therapy of granulocyte and monocyte absorption apheresis induces rapid remission in patients with ulcerative colitis.// Gastroenterology. 2003. 124. 4. Suppl 1. T. 1379.
28. Sandborn Q., Tremaine W., Offord K. et al. Transdermal nicotine for mildly to moderately active ulcerative colitis.// Ann. Intern. Med. 1997. 126. P. 364-371.
29. Sandborn W., Rachmilewitz D., Hanauer S. et al. Infliximab induction and maintenance therapy for ulcerative colitis: the Act 2 trial // Gastroenterology. 2005.128 (suppl. 2). A 688.
30. Sawada K., Kusugam K., Suzuki Y. et al. Multicenter randomized double blind controlled trial for ulcerative colitistherapy with leukocytapheresis // Gastroenterology. 2003. 124. 4. Suppl. 1.P.542.
31. Skelly M. M., Curtis H., Jenkins D. et al. Toxicity of mycophenolate mofetil (MMF) in patients with inflammatory bowel disease (IBD) // Gastroenterology. 2000. 14. P. 171-176.
32. Sutherland L.R., May G.R., Shaffer E.A. Sulphasalazine revisited: a meta-analysis of 5-minosalicylic acid in the treatment of ulcerative colitis.// Ann. Intern. Med. 1993. 118. P. 540-549.
33. Sutherland L., Roth D., Beck P. et al. Alternative to sulphasalazine: a meta-nalysis of 5-SA in the treatment of ulcerative colitis.// Inflam. Bowel Dis. 1997. 3. P. 665-678.
34. Tilg H., Vogelsang H., Ludwiczek O. et al. A randomized placebo-controlled trial of pegylated interferon alpha in active ulcerative colitis // Gastroenterology. 2003. 124. 4. Suppl. 1. P. 472.
35. Van Assche G., Noman M., Asnong K., Rutgeerts P. The use of the neurokinin-1 receptor Antagonist, SR-140333B, Nolpitantium Besilate, in mild to moderate active ulcerative colitis.// Gastroenterology. 2003. 124. 4. Suppl. 1. T 1377.
36. Wright J.P., Winter T.A., Candy S., Marks I. Sucralfate and methylprednisolone enemas in active ulcerative colitis - a prospective, single-blind study.// Dig. Dis. Sci. 1999. 44. 9. P. 1899-1901.
