Catad_tema Peptic ulcer - articles
Catad_tema Coagulopathy and bleeding - articles
Gastrointestinal bleeding
Published in the journal:"Doctor", N2, 2002 Ovchinnikov A., Doctor of Medical Sciences, Professor, MMA named after I.M.Sechenov
Gastrointestinal bleeding (GKB) is one of the most common causes of emergency hospitalization in surgical hospitals. The therapeutic task for bleeding from the gastrointestinal tract (GIT) is simple and logical: the patient's condition should be stabilized, the bleeding should be stopped, and treatment should be carried out, the purpose of which is to subsequently prevent episodes of GCC. To do this, it is necessary to establish the source of bleeding and its localization. Among the most serious mistakes, which can have very serious consequences, are underestimation of the severity of the patient's condition and the beginning of diagnostic and therapeutic manipulations without sufficient preparation of the patient. In order to correctly assess the volume of blood loss and the patient's condition, it is necessary to clearly understand what changes occur in the body with this pathology.
Pathophysiological disorders
Acute blood loss in GCC, as in any form of sufficiently massive bleeding, is accompanied by the development of a discrepancy between the reduced mass of circulating blood and the volume of the vascular bed, which leads to a drop in the total peripheral resistance (OPS), a decrease in the stroke volume of the heart (VOC) and the minute volume of blood circulation ( IOC), falling blood pressure. So there are violations of central hemodynamics. As a result of a drop in blood pressure, a decrease in blood flow rate, an increase in blood viscosity and the formation of erythrocyte aggregates in it, microcirculation is disturbed, and transcapillary metabolism changes. From this, in the first place, the protein-forming and antitoxic functions of the liver suffer, the production of hemostasis factors - fibrinogen and prothrombin is disrupted, the fibrinolytic activity of the blood increases. Microcirculation disorders lead to renal, lung, and cerebral dysfunction.
The body's defense reactions are primarily aimed at restoring central hemodynamics. The adrenal glands respond to hypovolemia and ischemia by releasing catecholamines, which cause generalized vasospasm. This reaction eliminates the deficit in filling the vascular bed and restores the OPS and UOS, which contributes to the normalization of blood pressure. The resulting tachycardia increases the IOC. Further, the reaction of autohemodilution develops, as a result of which fluid enters the blood from the interstitial depots, which replenishes the deficit in circulating blood volume (BCC) and dilutes stagnant, thickened blood. Central hemodynamics is stabilized, rheological properties of blood are restored, microcirculation and transcapillary metabolism are normalized.
Determination of the volume of blood loss and the severity of the patient's condition
The severity of the patient's condition depends on the amount of blood loss, however, when bleeding into the lumen of the stomach or intestines, it is not possible to judge the true amount of blood flowed out. Therefore, the amount of blood loss is determined indirectly, according to the degree of tension of the body's compensatory-protective reactions, using a number of indicators. The most reliable and reliable of them is the difference in BCC before and after hemorrhage. The original BCC is calculated from the nomogram.
Hemoglobin indirectly reflects the amount of blood loss, but is quite variable.
Hematocrit the number quite accurately corresponds to blood loss, but not immediately, since in the first hours after bleeding, the volumes of both formed elements and blood plasma proportionally decrease. And only after the extravascular fluid begins to penetrate into the bloodstream, restoring the BCC, the hematocrit falls.
Blood pressure. Loss of 10-15% of blood mass does not cause severe hemodynamic disturbances, since it can be fully compensated. With partial compensation, postural hypotension is observed. In this case, the pressure is maintained close to normal while the patient is lying, but it can fall catastrophically when the patient sits down. With more massive blood loss, accompanied by severe hypovolemic disorders, adaptive mechanisms are unable to compensate for hemodynamic disorders. Hypotension occurs in the supine position and vascular collapse develops. The patient goes into shock (pallor turning into slate-gray color, sweat, exhaustion).
Heart rate... Tachycardia is the first reaction to a decrease in the IOS to maintain the IOC, but tachycardia itself is not a criterion for the severity of the patient's condition, since it can be caused by a number of other factors, including psychogenic ones.
Shock index... In 1976, M. Algover and Burri proposed a formula for calculating the so-called shock index (Algover index), which characterizes the severity of blood loss: the ratio of heart rate and systolic blood pressure. In the absence of a BCC deficit, the shock index is 0.5. Its increase to 1.0 corresponds to a BCC deficit of 30%, and to 1.5-50% corresponds to a BCC deficit.
These indicators should be evaluated in conjunction with the clinical manifestations of blood loss. Based on the assessment of some of these indicators and the condition of patients, V. Struchkov et al. (1977) developed a classification that distinguishes 4 degrees of severity of blood loss:
I degree- general condition is satisfactory; moderate tachycardia; BP is not changed; Нb above 100 g / l; BCC deficit - no more than 5% of the due;
II degree: general condition - moderate, lethargy, dizziness, fainting, pallor of the skin, significant tachycardia, a decrease in blood pressure to 90 mm Hg; Hb - 80 g / l; BCC deficit - 15% of the due;
III degree- the general condition is severe; pale skin, cold, clammy sweat; the patient yawns, asks for a drink (thirst); pulse is fast, threadlike; BP is reduced to 60 mm Hg; Hb - 50 g / l; BCC deficit - 30% of the due;
IV degree- the general condition is extremely serious, bordering on agonal; prolonged loss of consciousness; pulse and blood pressure are not determined; BCC deficit - more than 30% of the due.
Patients with II-IV degrees of severity of blood loss require infusion therapy before starting diagnostic and therapeutic procedures.
Infusion therapy
With blood loss of no more than 10% of the BCC, blood transfusions and blood substitutes are not required. The body is able to fully compensate for this volume of the poured blood on its own. However, one should remember about the possibility of re-bleeding, which can quickly destabilize the patient's condition against the background of compensation stress.
Patients with significant acute GIQ, especially those in an unstable condition, should be admitted to the intensive care unit or intensive care unit. Constant access to the vein is required (catheterization of one of the central veins is desirable). Infusion therapy should be carried out against the background of constant monitoring of cardiac activity, blood pressure, renal function (amount of urine) and additional oxygenation.
To restore central hemodynamics, transfusion of saline, Ringer's solution, and basic solution is used. Medium-molecular polyglucin can be used as a colloidal blood substitute. Restoration of microcirculation is carried out using low molecular weight colloidal solutions (rheopolyglucin, hemodez, gelatinol). Blood is transfused to improve oxygenation (red blood cells) and clotting (plasma, platelets). So, with an active FSK, both are necessary, it is advisable to transfuse whole blood. With a stopped GCC, when the BCC deficit is replenished with saline solutions, to restore the oxygen capacity of the blood and stop the high degree of hemodilution, it is advisable to transfuse the erythrocyte mass. Direct blood transfusions are of primary importance for hemostasis. If clotting is impaired, which occurs in most patients with liver cirrhosis, it is advisable to transfuse fresh frozen plasma and platelet mass. The patient should receive fluid therapy until his condition stabilizes; in this case, the number of erythrocytes is required, which ensures normal oxygenation. With ongoing or re-emerging GCC, infusion therapy is continued until the bleeding stops completely and hemodynamic parameters stabilize.
Diagnosis of the causes of bleeding
First of all, it is necessary to establish whether the source of bleeding is in the upper or lower parts of the gastrointestinal tract. Bloody vomiting (hemotemesis) indicates the localization of bleeding in the upper sections (above the trait ligament).
Vomiting may be fresh, bright red blood, dark clotted blood, or so-called "coffee grounds". Red blood of different shades, as a rule, indicates massive bleeding in the stomach or bleeding from the veins of the esophagus. Pulmonary bleeding should be distinguished from gastric bleeding. The blood from the lungs is more scarlet, frothy, does not coagulate, is released when coughing. However, the patient can swallow blood from the lungs or from the nose. In these cases, typical bloody vomiting and even vomiting of "coffee grounds" is possible. Tarry sticky fetid stools (meleno), resulting from the reaction of blood with hydrochloric acid, the transition of hemoglobin to hydrochloric acid hematin and decomposition of blood under the action of intestinal enzymes, is a sign of bleeding in the upper gastrointestinal tract. However, there may be exceptions. Bleeding from the small and even from the large intestine can also be accompanied by melena, but in the presence of 3 conditions: 1) a sufficient amount of altered blood to make the stool black; 2) not too much bleeding; 3) delayed intestinal peristalsis, so that there is enough time for the formation of hematin. Bloody stools (hematochezia), as a rule, indicate the localization of the source of bleeding in the lower parts of the digestive tract, although with massive bleeding from the upper parts of the blood sometimes does not have time to turn into melena and can be released in a slightly changed form (Table 1).
Table 1. Clinical manifestations of gastrointestinal bleeding
| The nature of the bleeding | Possible reason |
| Vomiting of unchanged blood with clots | Rupture of varicose veins of the esophagus; massive bleeding from a stomach ulcer; Mallory-Weiss syndrome |
| Vomiting of "coffee grounds" | Bleeding from a stomach or duodenal ulcer; other causes of stomach bleeding |
| Tar stools (melena) | The source of the bleeding is most likely in the esophagus, stomach, or duodenum; the source of bleeding may be in the small intestine |
| Dark red blood evenly mixed with feces | The source of bleeding is most likely in the cecum or the ascending colon |
| Streaks or clots of scarlet blood in normal-colored feces | The source of bleeding is in the descending or sigmoid colon |
| Scarlet blood in the form of drops at the end of a bowel movement | Hemorrhoidal bleeding; anal fissure bleeding |
When the question arises about the localization of the GCC, it is first of all recommended to introduce the patient with a tube into the stomach. Blood aspirated through a tube confirms the localization of the bleeding source in the upper gastrointestinal tract. But a negative aspiration result does not always indicate the absence of bleeding in the upper digestive tract. Bleeding from a bulbous ulcer may not be accompanied by blood in the stomach. In such cases, the high localization of the source can be judged by other signs: the presence of hyperreactive intestinal noises and an increase in the content of nitrogenous compounds in the blood (primarily creatinine and urea). Nevertheless, the diagnosis of GCC is often very difficult, especially in the first hours after the onset of the disease, when the patient is already in serious condition, and there is no bloody vomiting and tarry stools have not yet appeared. If there is no clear idea of the presence and localization of its source, an endoscopic examination is performed.
Upper GI bleeding
They account for about 85% of all housing and communal services. In Moscow, according to A. Greenberg et al. (2000), bleeding of ulcerative etiology in 1988-1992. were observed in 10,083 patients, and in 1993-1998. - at 14 700, i.e. their frequency increased by 1.5 times. At the same time, the mortality rate of cooks in our country and abroad practically does not differ from the current rate 40 years ago; from 10 to 14% of patients die despite treatment (A. Greenberg et al., 1999; Y. Pantsyrev and D. Fedorov, 1999). The reason for this is an increase in the proportion of elderly and senile patients from 30 to 50%. Among them, the bulk are elderly patients taking non-steroidal anti-inflammatory drugs (NSAIDs) for joint pathology (E. Lutsevich and I. Belov, 1999). Mortality in patients over 60 years of age is several times higher than in young people. It is highest with bleeding from varicose veins of the esophagus - 60% (on average - 40%).
Especially high numbers are reached by mortality during emergency operations at the height of bleeding - it is 3 times higher than the current during operations performed after it was stopped. Thus, the first task of treating acute GIs is to stop bleeding and avoid emergency surgery. Its solution can be facilitated by empirical treatment, which does not require an accurate diagnosis that requires sufficiently invasive manipulations. Empiric treatment begins immediately after the patient is admitted to the intensive care unit against the background of infusion therapy. It acquires particular importance when it is impossible to urgently perform an endoscopic examination due to various reasons.
Empirical therapy consists in washing the stomach with ice water from the refrigerator and parenteral administration of drugs that reduce acidity. Strongly cooled fluid reduces blood flow in the stomach wall, and stopping bleeding, at least temporarily, is achieved in 90% of patients. In addition, lavage facilitates the emptying of the stomach from blood clots, which greatly facilitates subsequent gastroscopy. Parenteral administration of histamine receptor blockers and proton pump inhibitors has been substantiated, since, according to statistics, peptic ulcers are the most common cause of bleeding from the upper gastrointestinal tract. In addition, pepsin, which promotes platelet disaggregation, is inactivated at high gastric pH, which increases blood clotting while decreasing gastric acidity. Successfully conducted empiric therapy allows you to gain time and adequately prepare the patient for endoscopic examination and surgery.
Diagnostics of the causes of bleeding from the upper gastrointestinal tract
The key to the correct diagnosis even before the endoscopic examination can be given by a well-collected anamnesis. Has the patient had episodes of GCC before? Did he have a previously diagnosed stomach or duodenal ulcer? Does he present complaints specific to peptic ulcer disease? Was he previously operated on for peptic ulcers or portal hypertension? Does he have other diseases that could lead to bleeding, such as cirrhosis of the liver or coagulopathies? Does the patient abuse alcohol, regularly take aspirin or NSAIDs? Does he have nosebleeds? It is desirable to get an answer to these questions if the patient is conscious and sufficiently contact, for example, is not in a state of alcoholic intoxication.
Examination of the skin and visible mucous membranes reveals stigmata of liver cirrhosis, hereditary vascular anomalies, signs of capillarotoxicosis, paraneoplastic manifestations. Palpation of the abdomen may reveal tenderness (peptic ulcer), splenomegaly (cirrhosis of the liver or splenic vein thrombosis), and stomach swelling. Intraperitoneal bleeding (for example, in case of a disturbed ectopic pregnancy) sometimes manifests itself with signs of acute anemia similar to those of GCC. The presence of symptoms of peritoneal irritation, characteristic of bleeding into the abdominal cavity, can help in the differential diagnosis of these conditions. If abdominal auscultation reveals increased peristalsis, there is reason to assume that it is caused by blood entering the intestine from the upper gastrointestinal tract.
The most important information is given by esophagogastroduodenoscopy (EGDS); it allows not only to establish with a high degree of accuracy the localization of the source of bleeding and its nature, but also to carry out hemostatic measures, which in a significant number of cases make it possible to stop the bleeding. Radioisotope scanning (99 Tc-labeled colloidal sulfur or albumin) and angiography are very important in some situations, but they are not of great practical importance, since they can rarely be performed for emergency indications.
The main causes of bleeding from the upper gastrointestinal tract and their specific therapy
Rupture of varicose veins of the esophagus (GDP)
The cause of GDP is portal hypertension resulting from intrahepatic (cirrhosis, hepatitis) or extrahepatic blockade. Diagnosing GDP is not difficult; dilated and convoluted veins of a cyanotic hue, as a rule, are quite clearly visible during esophagoscopy, which should be carried out very carefully if GDP is suspected so as not to cause additional trauma to the thinned vein walls. Treatment of patients with GDP is the most important factor in reducing mortality in GCC. First aid consists in prolonged (1-2 days) tamponade of veins with a balloon probe and intravenous administration of 1% nitroglycerin solution (to reduce portal pressure) and vasopressin (pituitary gland preparation). This makes it possible to temporarily stop bleeding in about 60-80% of patients. If this measure is ineffective or there is a threat of recurrent bleeding, an attempt can be made to endoscopic sclerotherapy with intravenous or paravosal (which is safer) administration of sclerosants - 2% solution of thrombovar or varicocide, 1-3% solution of ethoxysclerol (polidocanol), cyanoacrylates (historyl, histoacryl, cyanoacrylates), fibrinkleber in a mixture with iodolipol in a 1: 1 ratio. In their absence, 96% ethyl alcohol is used.
Endoscopic treatment of GDP is indicated in patients over 60 years of age, previously operated on multiple times, with severe concomitant pathology. The conditions for the relatively safe conduct of medical esophagoscopy are stable hemodynamics and the absence of severe liver dysfunctions. Complications of GDP sclerotherapy are not uncommon. These include ulceration of the esophageal mucosa with bleeding, purulent thrombophlebitis, necrosis of the esophageal mucosa, and esophageal perforation. Mortality after emergency vein sclerotherapy against the background of ongoing bleeding reaches 25%, after planned sclerotherapy is significantly lower - 3.7%.
A promising method for the treatment of bleeding from the GDP is endovascular embolization of the esophageal veins. In combination with endoscopic sclerosis, it can reduce mortality in emergency cases to 6-7% (A. Scherzinger, 1999).
Bypass surgery (portocaval, splenorenal, mesocaval, and other anastomoses) is performed to direct blood from high-pressure esophageal veins to low-pressure systemic veins. However, at the height of bleeding, they are very risky. After shunting operations, the frequency of esophageal bleeding decreases, but mortality remains high - patients die not from bleeding, but from liver failure and encephalopathy caused by hyperammonemia. It is recommended to decompress only the esophageal and gastric veins by applying a selective distal splenorenal shunt.
Rupture of the mucous membrane of the cardiac stomach (Mallory-Weiss syndrome) observed with severe vomiting. The appearance of fresh blood during repeated vomiting suggests this pathology. Diagnosis is based on EGDS data. Bleeding can be quite intense, but often stops on its own with rest and hemostatic therapy. With continued bleeding, an attempt to electrocoagulate the bleeding vessels during endoscopy is justified. Occasionally there are indications for surgery (gastrotomy and suturing of vessels in the area of rupture).
Erosive esophagitis occurs with gastroesophageal reflux disease (GERD), which is very common. Often the basis of the disease is a hiatal hernia. Erosions in the cardiac esophagus can sometimes cause bleeding into the lumen of the esophagus and stomach and manifest, in addition to the classic symptoms of GERD (belching, heartburn, chest pain), vomiting mixed with blood.
Duodenal, gastric, or marginal (after gastric resection) ulcers are the cause of bleeding in 40-50% of patients. Ulcers on the posterior wall of the duodenal bulb are especially dangerous, since they can cause massive arterial bleeding as a result of arrosion of the branches of a large gastro-duodenal artery passing in this zone.
According to the widespread endoscopic classification of ulcerative bleeding according to Forrest, there are:
I. Continuous bleeding: A) profuse (jet); B) bleeding.
II. Past bleeding: A) high risk of recurrence (thrombosed vessel is visible); B) low risk of recurrence (presence of hematin on the defect).
III. Clinical signs of completed bleeding (melena) in the absence of endoscopic signs of bleeding from the detected source.
This classification allows you to determine the treatment tactics for bleeding ulcerative etiology. With profuse bleeding (IA), an emergency operation is indicated, since the use of conservative methods leads to a loss of time and worsens the prognosis. When blood is leaking from an ulcer (IB), attempts to stop bleeding through an endoscope by monoactive or bipolar electrocoagulation using high-frequency current, photocoagulation with an argon or YAG-neodymium laser, by argon-plasma coagulation with ionized gas or injecting the ulcer with ethyl alcohol are justified. bleeding ulcer through a catheter with a solution of caprofer - a carbonyl complex of ferric chloride and epsilon-aminocaproic acid. Occasionally, special endoclips are applied to the bleeding vessel. Using the entire set of endoscopic techniques listed above, according to Y. Pantsyrev and E. Fedorov (1999), persistent hemostosis was achieved in 187 (95%) of 206 patients. In 9 (4.6%) people, hemostasis was ineffective, the patients were urgently operated on. Emergency surgery is also indicated for recurrent bleeding that occurs in the next few hours after preliminary hemostasis.
If the bleeding has stopped with a high risk of recurrence (IIA according to Forrest), an urgent operation is indicated in the next day, as a rule, in the morning of the next day. The most justified surgical tactics for a bleeding gastric ulcer is its excision or suturing in combination with pyloroplasty and vagotomy (in the absence of signs of ulcer malignancy), and for duodenal ulcers - economical gastrectomy (antrumlectomy) or (in patients with a high degree of operational risk) - suturing ulcers with pyloroplasty and selective vagotomy (Yu. Pantsyrev, 1986, Yu. Pantsyrev and E. Fedorov, 1999).
Recurrent peptic ulcers after gastric resection relatively rarely are the cause of HCC. Usually they are located at the site of the gastro-jejunal anastomosis or near it, they arise, as a rule, due to the wrong choice of the method of surgery and technical errors in its implementation (Yu. Pantsyrev, 1986). Bleeding is especially persistent and intense in recurrent ulcers caused by hypergastrinemia with undiagnosed Zollinger-Ellison syndrome before surgery, if a section of the antrum of the stomach was left during resection. Reoperation in patients with a resected stomach is very difficult, therefore, they prefer conservative therapy and endoscopic methods of hemostasis. In general, the choice of treatment tactics is determined by the intensity of bleeding; the principles of treatment do not differ from those in non-operated patients.
Sometimes erosive-ulcerative bleeding occurs due to solitary ulceration described by Dielafoy. These are small superficial ulcers, at the bottom of which there is a rather large artery. Arrosion of the latter leads to profuse, sometimes fatal gastric bleeding. According to many authors, the disease is based on aneurysms of small arteries of the submucous layer of the stomach. It is not excluded that the disease is caused by a congenital malformation of blood vessels. Not the least role in its pathogenesis is played by the peptic factor, mechanical damage to the mucous membrane, pulsation of the underlying arteries, hypertension and atherosclerosis. Dielafoy's solitary ulceration (SID) is usually located in the cardiac part of the stomach parallel to the lesser curvature, retreating by 3-4 cm.
The disease usually presents with sudden massive bleeding. Conservative therapy for SID is most often unsuccessful, almost all patients die from blood loss (A. Ponomarev and A. Kurygin, 1987). Surgical treatment consists in suturing the stomach wall to the muscle layer with ligation of a bleeding artery or in excision of pathological areas of the gastric wall within healthy tissues. Vascular embolization may be effective.
Acute hemorrhagic gastritis usually associated with medication (aspirin, NSAIDs) and alcohol. Hemorrhagic gastritis is often erosive in nature and often develops as a stressful condition in patients with sepsis, burns, severe concomitant trauma, peritonitis, acute respiratory failure, myocardial infarction, as well as after severe surgical interventions in the early postoperative period. Differential diagnosis of acute bleeding gastric ulcers with hemorrhagic gastritis is possible only with the help of endoscopic examination. It is very difficult to stop bleeding in acute hemorrhagic gastritis, since, as a rule, large areas of the gastric mucosa are bleeding intensively. Preventive and therapeutic parenteral use of antacids and H-blockers, gastric lavage with ice solutions, irrigation of the mucosa during endoscopy with caprofer solution, intravenous administration of hemostatic agents, inhibitors of fibrinolysis and vasopressin, transfusion of fresh blood and platelet mass are important.
The reason from 3 to 20% of all housing complexes are decaying tumors of the stomach. In most cases, such bleeding is characterized by moderate blood loss, often stops on its own, but then can resume again. Bloody vomiting and classic melena are not as common as with bleeding ulcers, but the stool may turn dark. The diagnosis is established or clarified with EGDS. With advanced cancers, erased, atypical symptoms are possible. In the diagnosis of complicated cases, in addition to endoscopic examination, the role of abdominal radiography is important.
Emergency assistance consists in endoscopic electro- or photocoagulation with a laser, cauterization of concentrated caprofer solution. Subsequently, as well as with the ineffectiveness of hemostatic therapy, surgical intervention is indicated, the volume of which depends on the localization of the tumor and the stage of the cancer process.
Stomach polyps rarely cause acute bleeding. Massive bleeding is more common with such benign tumors as leiomyoma, neurofibroma, etc. Moreover, they can be their first manifestation (Yu. Pantsyrev, 1986).
Hemobilia, hematobilia- the release of blood from the biliary tract. Arteriobiliary fistulas are formed due to trauma, liver biopsy, hepatic abscesses, cancer, hepatic artery aneurysm. Often, there is a combination of signs of gastrointestinal tract with hepatic colic and jaundice. With EGDS, the presence of blood in the duodenum and its release from the nipple of Vater is noted. As a therapeutic measure, selective embolization of the hepatic artery can be recommended, and if ineffective, its ligation.
Gastrointestinal endometriosis is quite rare. The diagnosis can be made by repeated GCC that occur synchronously with menstruation. The appearance of melena or dark stools or hematochezia is preceded by abdominal pain. Endoscopic examination should be performed at the height of bleeding, but it is extremely rare to detect a bleeding area of the gastric or intestinal mucosa during endoscopy or colonoscopy. With age, such bleeding decreases and stops in menopause.
Aneurysms of the aorta and branches of the celiac artery can give massive, often fatal bleeding when ruptured. They are usually preceded by small prodromal bleeding - "harbingers". Described are duodenal bleeding as a result of aortointestinal fistula in case of anastomotic leak after aortic replacement due to its atherosclerotic lesion and Leriche syndrome.
Bleeding from the lower gastrointestinal tract
In 15% of cases, GCC occurs below the tract ligament, in 1% of cases - in the small intestine, in 14% - in the colon and rectum.
Diagnostics. Careful questioning of the patient and a well-collected anamnesis can provide important information (Table 2). If there is blood in the stool, it is important to find out whether the blood is mixed with feces (the source is located high) or is released in a relatively unchanged form at the end of defecation, which is more typical for low-lying bleeding tumors and hemorrhoids.
Table 2. Diagnostic value of pain syndrome in case of bleeding from the lower gastrointestinal tract (A. Sheptulin, 2000)
Palpation of the abdominal cavity and digital examination of the anus are required in all patients. Digital rectal examination, according to statistics, can reveal up to 30% of all colon tumors, including those complicated by bleeding. The next stage of diagnostics is anoscopy and rectosigmoscopy, the effectiveness of which in cancer of the colon is 60%. In the presence of tarry stools, which may result from both gastroduodenal bleeding and bleeding from the ileum and right colon, nasogastric aspiration through a tube and EGD is recommended to exclude pathology of the stomach and duodenum. Colonoscopy is the most informative method for diagnosing colonic pathology, but with heavy bleeding, it is rather difficult to perform it. If the bleeding stops at least for a while, then with the help of this procedure a wide variety of pathologies, including vascular ones, can be diagnosed.
Mesenteric arteriography in intestinal bleeding allows to identify the extravasation of contrast and to determine the side and approximate localization of the source of bleeding. Angiography is the only method for diagnosing bleeding in the small intestine, it makes it possible to inject vasopressin directly into the bleeding artery. Extravasation is determined only with sufficiently massive bleeding, but even in the absence of its signs, arteriogrophy can detect vascular pathology that is the cause of bleeding. Scintigraphy with 99 Tc-labeled erythrocytes or radioactive In-labeled platelets is a more sensitive method; the source of bleeding is detected even at a relatively low intensity, but scintigraphy takes a lot of time and therefore can hardly be considered a method of emergency diagnosis. Contrast methods of X-ray examination (irrigoscopy and irrigography) are not able to identify the source of bleeding, but can help in the diagnosis of tumor, diverticulosis, intussusception and other diseases complicated by bleeding.
The main causes of bleeding from the lower gastrointestinal tract and their specific therapy
One of the most common causes of hematochezia in elderly patients is colon diverticulosis. The frequency of this pathology increases with age; after 70 years, diverticula are found during colonoscopy in every 10th patient. The formation of diverticula is facilitated by a sedentary lifestyle, dysfunction of the colon (tendency to constipation), intestinal dysbiosis, Bleeding, often massive, complicate the course of diverticulosis in 10-30% of cases. It is believed that diverticula are more often localized in the descending and sigmoid colon, but they also occur in the transverse colon and in the right half of the colon. Bleeding in diverticulosis may be preceded by abdominal pain, but it often begins suddenly and is not painful. The outflow of blood can stop on its own and recur after a few hours or days. In almost half of cases, bleeding occurs once.
Conservative therapy (transfusion of fresh blood, platelet mass, administration of α-aminocaproic acid, decinone, administration of vasopressin into the mesenteric artery during angiography) is effective in most patients. In some clinics, transcatheter embolization is used after angiography (A. Sheptulin, 2000). If a source of bleeding is found during colonoscopy, which is quite rare, one can also count on the effect of local hemostatic measures (electrocoagulation, irrigation with caprofer). With ongoing or recurrent bleeding, one has to resort to surgical intervention (resection of the colon, the volume of which is smaller, the more accurate the topical diagnosis).
At colon polyps occasionally bleeding occurs in cases of spontaneous detachment of the leg of the polyp, or - much more often - with inflammation and ulceration of its surface.
Massive bleeding from decaying colon cancer is very rare. More often there are chronic intermittent bleeding in the form of small "spits" of blood, sometimes mixed with mucus or - with a high location of the tumor - with a change in the color and consistency of feces.
Bleeding of moderate to low intensity is possible with nonspecific colitis(ulcerative colitis and Crohn's disease), intestinal tuberculosis and acute infectious colitis. These diseases are characterized by abdominal pain preceding the appearance of blood, which is usually mixed with mucus. In the diagnosis and differential diagnosis of colitis bleeding, an important role is played by colonoscopy, which makes it possible to identify differences in the endoscopic manifestations of certain diseases. The morphological examination of biopsies of the intestinal wall helps to clarify the diagnosis.
Embolism and thrombosis of mesenteric vessels with their otherosclerotic lesion in the elderly, endarteritis and systemic vasculitis in younger patients, embolism from the cardiac cavities (with myocardial infarction, heart defects) or from the aorta (with its atherosclerotic lesion) can cause acute disorders of mesenteric circulation, ischemic lesions and hemorrhagic infarction intestines, manifested by the release of a fairly large amount of altered blood. Such bleeding is characterized by a pre-existing severe pain syndrome, nausea, vomiting, sometimes a collaptoid state, and as the disease progresses, an increase in symptoms of intoxication, peritoneal phenomena.
In case of hemorrhagic infarction of the colon, depending on the stage of the disease, colonoscopy reveals large areas of edematous, cyanotic or blood-soaked mucosa with increased bleeding, multiple submucosal hemorrhages. Later, superficial bleeding ulcerations appear, areas of necrosis may occur, followed by tissue decay and perforation. With high occlusion of the superior mesenteric artery, infarction and necrosis of the entire small intestine and the right half of the large intestine are possible; with thrombosis of the inferior mesenteric artery due to the presence of powerful vascular colloterals, infarction is usually limited to the sigmoid colon.
In difficult diagnostic situations, angiography is very useful - the nature of the blood flow disturbance, the localization and length of occlusion, and the presence of collaterals are precisely established. If an intestinal infarction is suspected, laparoscopy provides important diagnostic information.
Treatment of patients with intestinal bleeding against the background of acute disorders of the mesenteric circulation, as a rule, is operative. Since blood in the lumen of the intestine usually appears at the stage of intestinal infarction, which indicates decompensation of mesenteric circulation, resection of irreversibly changed sections of the intestine is performed, which is complemented by intervention on the mesenteric vessels in order to restore blood circulation in viable remaining sections (V. Saveliev and I. Spiridonov, 1986) ...
Quite a rare cause of intestinal bleeding - hemorrhagic angiomatosis colon and small intestine, which causes angiodysplasia, known as disease (syndrome) Randu-Osler-Weber. Diagnostics is facilitated by modern high-resolution video colonoscopy, which makes it possible to detect even small changes in the vascular pattern of the mucous membrane.
Capillary and cavernous hemangiomas and angiodysplasias of the small and large intestine(arteriovenous malformations), according to A. Sheptulin (2000), are the cause of massive intestinal bleeding in 30% of cases. Clinically, the disease is manifested mainly by bleeding from the rectum during bowel movements and regardless of it. With cavernous hemangiomas, massive bleeding is possible, accompanied by collapse. Occasionally, there is pain in the lower abdomen, worse before bleeding. For rectal angiomas, false urge to defecate, a feeling of incomplete emptying, and sometimes constipation occur. Differential diagnosis with other causes of hematochezia, especially bleeding nonspecific colitis, intestinal tuberculosis, hemorrhoids, is very difficult.
The main role in the diagnosis of colon hemongiomas is played by rectosigmoscopy and colonoscopy. Endoscopic examination reveals a bluish-purple color of the intestinal mucosa in a limited area, the absence of typical folding, dilated, convoluted, bulging vessels that form an irregular plexus, clearly delimited from unchanged areas of the mucous membrane. A biopsy of such formations can lead to massive bleeding, which can be very difficult to stop. The main and most radical method of treating intestinal hemangiomas is surgical, although, according to V. Fedorov, treatment tactics require a differential approach. With the development of massive bleeding from low-lying hemangiomas, M. Anichkin et al. (1981) performed embolization and ligation of the superior rectal artery, which stopped bleeding, albeit temporarily. With insignificant and periodically repeated bleeding, which does not affect the general condition of the patient, expectant tactics are permissible. After the cessation of blood flow, small angiomas of the distal colon can be removed by electro excision or sclerotherapy.
The most common cause of rectal bleeding is haemorrhoids. More than 10% of the adult population suffers from hemorrhoids, the release of fresh blood from the rectum is one of its main symptoms. Red blood with hemorrhoids usually becomes noticeable at the end of the act of defecation. The feces retain their normal color. Bleeding can be accompanied by pain and a burning sensation in the anus, which intensify during and after bowel movements. Often hemorrhoids fall out when straining. With massive hemorrhoidal bleeding, active hemostatic therapy is required. In case of repeated bleeding, oral glyvenol is recommended (1 capsule 4 times a day) and suppositories with thrombin or adrenaline. It is possible to use injections of sclerosing drugs. Various types of hemorrhoidectomy are a radical method of treatment. A similar clinical picture is given by crack in the anus. For differential diagnosis with hemorrhoidal bleeding, as a rule, digital rectal examination and anoscopy are sufficient.
Significant bleeding in childhood can be caused by mucosal ulceration Meckel's diverticulum. The clinical picture is very similar to the manifestations of acute appendicitis, the diagnosis in most patients is established during appendectomy. In children of the first 2 years of life, the discharge from the anus of a portion of blood with mucus (having the appearance of raspberry jelly), combined with anxiety and crying, is the main symptom of intussusception of the large intestine, an acute disease that is very common at this age. For its diagnosis, and sometimes for treatment, air irrigoscopy is used (dosed introduction of air into the large intestine under the control of an X-ray screen).
- the outflow of blood from the lower parts of the digestive tract. It is manifested by symptoms of the underlying disease, as well as the presence of fresh blood during bowel movements (mixed with feces or located in the form of clots on the feces). For diagnostics, rectal digital examination, endoscopy of the small and large intestine, angiography of mesenteric vessels, scintigraphy with labeled erythrocytes, clinical and biochemical blood tests are used. Treatment is usually conservative, including therapy for the underlying disease and blood loss replacement. Surgical treatment is required for severe intestinal damage (thrombosis, vascular ischemia, necrosis).

General information
Intestinal bleeding is bleeding that occurs into the lumen of the small or large intestine. Intestinal bleeding accounts for about 10-15% of all bleeding from the digestive tract. Usually they do not have obvious clinical symptoms, do not lead to hemorrhagic shock. Most often, the fact of intestinal bleeding is revealed by chance during an examination for other diseases. The level of bleeding can be determined by the color and consistency of feces: intestinal bleeding from the small intestine is manifested by liquid, black, fetid feces; blood from the upper colon is dark, evenly mixed with feces. In the presence of intestinal bleeding from the lower parts of the colon, scarlet blood envelops the stool from above. Minor bleeding may not manifest clinically in any way; they can only be detected by performing an analysis of feces for occult blood.
Causes of intestinal bleeding
The cause of bleeding can be a variety of diseases of the intestines and mesenteric vessels. Angiodysplasia of the vessels of the small and large intestine can manifest itself only with bleeding and have no other clinical signs. Bowel diverticulosis is the most common cause of bleeding. Also, intestinal bleeding is often accompanied by chronic (Crohn's disease, ulcerative colitis) and acute inflammatory bowel diseases (pseudomembranous colitis); specific pathology of the small or large intestine (tuberculous colitis).
Also, intestinal bleeding can be caused by lesions of the mesenteric vessels - intestinal ischemia due to spasm or thrombosis of the mesenteric arteries. Tumor pathology (cancer, intestinal polyps) ends with massive bleeding. The source of intestinal bleeding can be hemorrhoids, anal fissures. In children, a common cause of intestinal bleeding is foreign bodies in the digestive tract.
More rare factors that provoke intestinal bleeding include radiation colitis after radiation therapy, aorto-intestinal fistulas, ankylostomiasis, intestinal syphilis, amyloidosis, long marathon races in athletes. In less than 10% of cases, it is not possible to identify the cause of intestinal bleeding.
Intestinal bleeding symptoms
Intestinal bleeding is rarely massive, causing an obvious clinic of hypovolemia, hemorrhagic shock. Quite often, patients mention the periodic appearance of blood in the stool only after a thorough history taking. The most common complaint in intestinal bleeding is the discharge of blood in the feces. When bleeding from the small intestine, the blood is in contact with digestive enzymes for a long time, which leads to the oxidation of hemoglobin and gives the blood a black color. If there is a lot of blood, it irritates the intestinal walls and leads to an increase in the passage of contents through the digestive tube. This is manifested by the presence of a liquid, black, fetid stool - melena.
If the source of bleeding is in the upper parts of the large intestine, the blood takes an active part in the process of the formation of fecal masses, has time to oxidize. In such situations, an admixture of dark blood is found, evenly mixed with feces. In the presence of intestinal bleeding from the sigmoid rectum, the blood does not have time to mix with the feces, therefore it is located on top of the externally unchanged feces in the form of drops or clots. The color of blood in this case is scarlet.
If the source of bleeding is colon diverticula or angiodysplasia, bleeding may occur against the background of complete health, not accompanied by pain. If intestinal bleeding has developed against the background of inflammatory, infectious intestinal pathology, the appearance of blood in the stool may be preceded by abdominal pain. Pain in the perineum during bowel movements or immediately after it, combined with the appearance of scarlet blood in the stool or on toilet paper, is characteristic of hemorrhoids and cracks in the anus.
Infectious pathology of the large intestine, which led to the development of intestinal bleeding, may be accompanied by fever, diarrhea, and constant urge to defecate (tenesmus). If intestinal bleeding has occurred against the background of a long-term subfebrile condition, significant weight loss, chronic diarrhea and intoxication, you should think about intestinal tuberculosis. Intestinal bleeding, combined with signs of systemic damage to the skin, joints, eyes and other organs, is usually a symptom of nonspecific inflammatory bowel disease. In the presence of stained feces and the complete absence of bleeding clinics, it is necessary to find out whether the patient has consumed dishes with food dyes that could lead to a discoloration of the feces.
Diagnosis of intestinal bleeding
To accurately establish the fact of intestinal bleeding, not only the consultation of a gastroenterologist, but also an endoscopist is required. To establish the severity and risk of an unfavorable outcome in intestinal bleeding, a clinical blood test is performed on an emergency basis (the level of hemoglobin, erythrocytes, normocytes, hematocrit is determined), an analysis of feces for occult blood, a coagulogram. During the examination, the gastroenterologist pays attention to the pulse rate, blood pressure level. It is imperative to find out if the patient has a history of episodes of loss of consciousness.
If there is scarlet blood in the stool, a digital examination of the rectum is carried out for the presence of hemorrhoids, polyps. However, it should be remembered that confirmation of the diagnosis of hemorrhoidal enlargement of the rectal veins does not exclude intestinal bleeding from other parts of the digestive tube.
The simplest and most affordable method to identify the source of intestinal bleeding is endoscopic. To establish a diagnosis, colonoscopy (examination of the upper colon), sigmoidoscopy (visualization of the sigmoid and rectum) can be performed. An endoscopic examination allows to identify the cause of intestinal bleeding in 90% of cases, to carry out simultaneous endoscopic treatment (polypectomy, electrocoagulation of a bleeding vessel). Close attention is paid to the description of bleeding (stopped or ongoing, the presence of a blood clot and its characteristics).
If bleeding continues, and its source could not be identified, mesentericography, mesenteric vessel scintigraphy using labeled erythrocytes is performed. Mesentericography reveals the source of intestinal bleeding in 85% of cases, but only when its intensity is more than 0.5 ml / min. The contrast injected into the mesenteric vessels comes out with the blood flow into the intestinal lumen, which can be seen on an X-ray. In this case, a catheter located in the mesenteric vessels can be used to harden them or administer vasopressin (it will cause vasoconstriction and stop bleeding). This method is most relevant in identifying intestinal bleeding against the background of intestinal diverticulosis, angiodysplasia.
If the intensity of intestinal bleeding is low (0.1 ml / min.), Scintigraphy with labeled erythrocytes will help to identify its source. This technique requires a certain amount of time and preparation, however, with high accuracy it makes it possible to diagnose low-intensity intestinal bleeding. Unlike mesentericography, scintigraphy can identify the source of bleeding, but not the cause.
Prediction and prevention of intestinal bleeding
It is very difficult to predict the outcome of intestinal bleeding, since it depends on many factors. Mortality from intestinal bleeding varies from country to country, but remains quite high. In the United States, for 8 years, starting in 2000, intestinal bleeding as the cause of death was recorded in almost 70,000 cases. Prevention of intestinal bleeding includes the timely detection and treatment of diseases that can lead to this complication.
In this article, you will learn: what is intestinal bleeding. Causes and treatment.
Date of publication of the article: 05/22/2017
Date the article was updated: 05/29/2019
Intestinal bleeding is the discharge of blood into the lumen of the small or large intestine. Blood is released from the damaged intestinal wall and sooner or later leaves the body naturally during a bowel movement. Moreover, the nature of the blood in the stool will be very different depending on or localization or "height" of the site of mucosal damage. The higher the secretion of blood begins in the gastrointestinal tract, the more altered blood will be in the stool. It is by the unusual appearance and color of feces that the patient may suspect that something is wrong with the intestines.
Intestinal bleeding is only a symptom or manifestation of a disease, some of which are deadly. That is why the slightest suspicion of the release of blood from the intestines should be the reason for going to the doctor. The primary link in the diagnosis is most often the therapist, who, as necessary, refers the patient to a surgeon, proctologist, gastroenterologist or oncologist.
The prognosis of the disease depends entirely on the massiveness of the bleeding, as well as the immediate cause of this condition. In some cases, the disease can disappear without a trace, and sometimes it threatens the patient's life. Approximately 60-70% of the cause of gastrointestinal bleeding is gastric ulcer and duodenal ulcer - without immediate help, such conditions can take the life of a patient in a matter of hours.
Causes of intestinal bleeding
The main reasons for the flow of blood from the intestines:
- Peptic ulcer of the stomach and duodenum is the most common cause of the appearance of altered blood in the stool.
- Diseases of the rectum: anal fissure, hemorrhoids.
- Bowel Injury: The rectum can be injured by a fall or by a foreign object. The rest of the gastrointestinal tract can be damaged by foreign objects accidentally or intentionally swallowed by the patient: needles, hairpins, blades, and so on.
- A special group of inflammatory bowel diseases: Crohn's disease, ulcerative colitis, celiac disease and others.
- Intestinal infections caused by a special group of intestinal microbes: dysentery, shigellosis, typhoid fever.
- Oncological diseases of the intestine: intestinal cancer of various localization.
 Polyps (abnormal tissue overgrowth) can also cause intestinal bleeding.
Polyps (abnormal tissue overgrowth) can also cause intestinal bleeding. Intestinal bleeding symptoms
With massive bleeding, the picture of the disease is so vivid that the diagnosis of such a condition is not difficult. The situation is worse with diagnostics for rare and minor bleeding.
We list what the symptoms of intestinal bleeding are.
Direct detection of blood in the stool
Doctors call this blood fresh because its appearance has not changed. Fresh blood usually covers the surface of the faeces or is excreted at the same time as stool. This symptom is typical for diseases of the lowermost parts of the large intestine of the rectum. Hemorrhoids, fissured anus, rectal cancer and rectal inflammation - proctitis - are very often accompanied by the appearance of fresh blood in the stool.
Streaks of blood in the feces
The blood retains its appearance, but it is already mixed with feces or has the appearance of streaks. This symptom is also typical for diseases of the large intestine, but at the same time, the "higher" parts of the large intestine are affected: the cecum and sigmoid colon.
The cause may be colon cancer and a special group of inflammatory diseases of the colon - colitis, including Crohn's disease or ulcerative colitis (ulcerative colitis). Also, blood in the stool can occur against the background of some infectious diseases - dysentery and shigellosis.
Changes in color, odor and consistency of stool
The feces acquire a liquid or mushy consistency, black color, "varnished" surface and a very characteristic fetid odor. Doctors call this stool tarry feces or chalk. Such a stool occurs due to the fact that the enzyme systems of the stomach and intestines "digest" the blood, releasing iron from it, which determines the same black as tar color. This is one of the most characteristic symptoms of gastric or small intestinal bleeding accompanying gastric ulcer and duodenal ulcer, as well as malignant neoplasms of these parts of the gastrointestinal tract.
There is a small nuance - melena can accompany not only gastrointestinal bleeding, but also the outflow of blood from the oral cavity, esophagus, nasopharynx and upper respiratory tract. In this case, the patient simply swallows blood, which undergoes all the same enzymatic reactions in the stomach and intestines.
The second caveat is that feces can acquire a dark hue when taking certain foods and medications: raw meat, activated carbon, bismuth and iron preparations. This feature is described in the "Side Effects" section of each drug, but it still scares patients. In fact, such feces are fundamentally different from true melena, primarily in the absence of odor and varnished shine.
Stomach ache
Abdominal pain often accompanies the initial period of the condition. Pain syndrome has its own characteristics depending on the root cause and localization of bleeding:
- with bleeding duodenal ulcers, the pain is very strong and sharp;
- with oncological diseases of the intestine - dull and fickle;
- with ulcerative colitis - migratory, cramping;
- with dysentery, an accompanying urge to defecate.

Weight loss
Weight loss is also a very characteristic symptom that accompanies intestinal bleeding. This is due to the constant loss of iron and nutrients in the blood, as well as the disruption of the damaged intestine. The destruction of the intestinal mucosa interferes with the absorption of nutrients from food.
Anemic conditions
Anemia or anemia is a decrease in the level of red blood cells, erythrocytes and hemoglobin. Due to blood loss, the body does not have time to restore iron stores and synthesize new hemoglobin and red blood cells. With a massive outflow of blood, anemia occurs acutely and leads to a violation in all organs and tissues. With periodic losses of small amounts of blood, anemia develops slowly. Such latent anemias also harm a person's health, reduce his ability to work and resist other diseases.
Anemia can be diagnosed by a general blood test, but it can be assumed by indirect signs: pallor of the skin and mucous membranes, weakness, drowsiness, dizziness, dry skin and hair, brittle nails, shortness of breath and palpitations - tachycardia.
Indigestion
Digestive disorders are not direct signs of intestinal bleeding, but they often accompany them. This can include diarrhea, constipation, bloating, gas, nausea and vomiting.
Fever
An increase in temperature is characteristic of some diseases that accompany intestinal bleeding: dysentery, shigellosis, NUC, Crohn's disease and other inflammatory bowel diseases.
Paraneoplastic Syndrome
With cancer of the intestine, a special symptom complex can develop - paraneoplastic syndrome, that is, a list of symptoms that accompanies any malignant process: weakness, dizziness, lack or perversion of appetite, sleep and memory disorders, itching and vague rashes, specific changes in the blood test picture.
Diagnostic measures for intestinal bleeding
It is very important to recognize this condition in time, because even small blood loss significantly impairs the patient's working capacity and quality of life. We list the obligatory minimum of studies for intestinal bleeding.
Endoscopic diagnostics
Colonoscopy - isolated or in combination with fibrogastroscopy - is an examination of the inner surface of the gastrointestinal tract using an endoscope. An endoscope is a long, thin and flexible tube equipped with fiber optics and connected to a monitor screen. The tube can be inserted through the mouth or through the patient's anus. During endoscopy, you can not only identify the source of bleeding, but also "cauterize" this place or put metal brackets on it with special attachments, and also take a suspicious bleeding area of the mucous membrane for biopsy and subsequent examination under a microscope.
 Colonoscopy
Colonoscopy X-ray methods
X-ray examination of the intestine is carried out with a passage of barium. This rather old research method has been partially replaced by endoscopy. However, X-ray remains informative, especially in cases where endoscopy is impossible for technical and physiological reasons.
The method consists in the fact that the patient receives a solution of barium salt in the form of a drink or enema. Barium solution is clearly visible on x-ray. It tightly fills the intestinal lumen, repeating its internal relief. Thus, you can see the characteristic changes in the mucous membrane of the digestive tract and suggest the cause of the bleeding.
Microscopic examination
Histological or microscopic examination of the obtained fragments of the mucous membrane. With the help of a biopsy, you can confirm or deny malignant tumors, as well as various inflammatory bowel diseases. Histology is the gold standard for the diagnosis of Crohn's disease and ulcerative colitis.
Rectoscopy
This is an examination of the rectum using a digital method or a special rectal speculum. It is a quick and easy way to detect abnormal hemorrhoidal veins, fissures and tumors of the rectum.
 Rectoscope - a tool with which the doctor examines the rectum
Rectoscope - a tool with which the doctor examines the rectum Laboratory diagnostics
- A blood test to monitor the level of hemoglobin, erythrocytes and platelets. The first two indicators provide information about the nature and severity of blood loss, and the platelet level will indicate the patient's individual problems with blood clotting.
- Analysis of feces for various indicators: microbial composition in intestinal infections, the remains of undigested fibers, as well as analysis of feces for occult blood. The latter analysis is extremely important for the diagnosis of rare and minor bleeding, when those small amounts of lost blood do not alter the appearance of feces in any way. Such an analysis is performed for clinical symptoms of intestinal bleeding and for any unclear anemia.
- Special blood tests for antibodies to various infectious and nonspecific intestinal diseases.
Treatment of intestinal bleeding
The speed, duration and aggressiveness of therapy directly depend on the severity of bleeding, as well as on its root cause.
- Massive bleeding from any part of the intestine that threatens the patient's life is subject to immediate surgical treatment. First of all, they try to stop the blood by endoscopic methods: by cauterization or the imposition of staples or clips on a bleeding vessel. If such a gentle treatment is impossible or ineffective, doctors go for open surgery. Such surgical treatment is urgent.
- Replenishment of blood volume by transfusing donor blood components or blood substitute solutions. Such actions are absolutely necessary to stabilize the patient's condition after massive bleeding.
- Planned surgical treatment involves a certain amount of surgical intervention in the preliminary preparation of the patient. Such planned operations include surgical treatment of hemorrhoids, removal of intestinal polyps or tumors, plastics of gastric or duodenal ulcers.
- Medicinal stopping of bleeding with hemostatic or hemostatic drugs: tranexam, ethamsylate, aminocaproic acid, calcium gluconate and others. This treatment is used only for minor bleeding.
- Treatment of the immediate cause of bleeding: This includes a strict diet and antiulcer therapy, specific treatment for ulcerative colitis, and antibiotic therapy for intestinal infections. In these cases, cure or at least stabilization of the cause of bleeding completely eliminates blood loss.
- Taking iron preparations to restore hemoglobin levels and treat anemia is indicated for all patients after intestinal bleeding.
 Hemostatic drug Tranexam
Hemostatic drug Tranexam Disease prognosis
The prognosis with the correct and timely treatment of intestinal bleeding is successful.
The highest mortality rate and severe health consequences are caused by intestinal bleeding from ulcers of the stomach and duodenum.
Also, the prognosis for the patient's life with bleeding from a disintegrating intestinal cancer is extremely unfavorable. Such cancer is often neglected and cannot be radically cured.
From this article you will learn about the causes, manifestations, methods of detection and treatment of a formidable complication of various pathological conditions of the gastrointestinal tract - bleeding. Depending on the location, there is gastric, intestinal, esophageal bleeding.
Date of publication of the article: 11.02.2017
Date the article was updated: 05/29/2019
Gastric bleeding - the expiration of blood into the lumen of the stomach. The exact source of bloody discharge can only be established using special research methods, therefore the term "gastrointestinal bleeding" is used.
The gastrointestinal tract is conventionally divided into two sections: upper and lower. The upper includes: the esophagus, stomach, duodenum.
This article focuses on bleeding in the stomach, since 80–90% of all bleeding in the digestive system occurs here. The stomach accounts for half of them.
Bleeding begins due to the destruction of the surface of the mucous membrane of the organ, or rupture, or arrosion (tissue erosion) of the vessel wall. Sometimes the cause of bleeding can be eliminated completely, sometimes - only to keep the patient in a satisfactory condition.

Which doctor to contact:
- Acute profuse bleeding requires urgent hospitalization and treatment in a surgical hospital. Also, the surgeon is consulted with bloody discharge from the rectum.
- For symptoms of diseases of the digestive system, they receive treatment from a therapist or gastroenterologist.
- The presence of bleeding, bruising, petechiae (spots on the skin caused by capillary hemorrhage) is a reason to consult a hematologist (blood specialist).
- The occurrence of common oncological signs - extreme exhaustion, pain, changes in appetite - requires examination by an oncologist.
Anything is dangerous. Absence or delayed treatment can be fatal.
Types of gastric bleeding
Causes leading to stomach bleeding
There are more than 100 possible processes and pathologies leading to the destruction of the walls of blood vessels.
The main 4 groups:
1. Diseases of the gastrointestinal tract

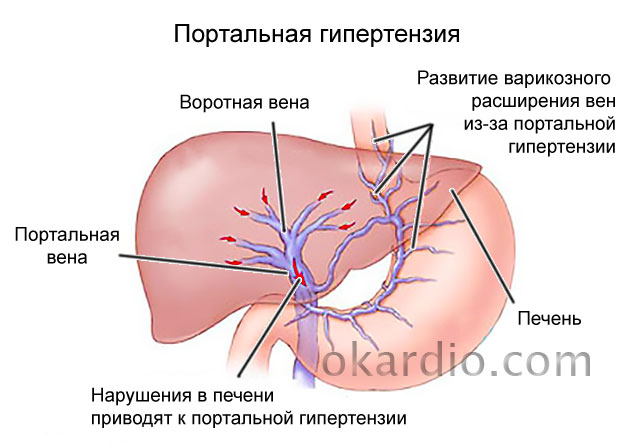
2. Bleeding due to portal hypertension
- Chronic hepatitis;
- cirrhosis of the liver;
- blockage of the portal or hepatic veins;
- reduction of the section of veins due to the action of tumors, scars.
3. Damage to blood vessels

4. Pathology of blood and hematopoiesis
- Aplastic anemia;
- hemophilia;
- thrombocytopenia;
- leukemia;
- hemorrhagic diathesis.
 Click on the photo to enlarge
Click on the photo to enlarge A combination of two or more factors is often observed.
Symptoms of gastric bleeding
The type of signs that occur in the presence of open blood flow in the stomach, and the power of their manifestation are determined by the size of the open wound and the duration of the process.
Common symptoms of gastric bleeding are associated with decreased blood supply to the organs. Nonspecific signs characteristic of internal hemorrhage in any cavity of the body:
- weakness, sluggish response to what is happening, up to fainting with massive bleeding;
- pallor of the skin, cyanosis (blueing) of the fingers, nose, nasolabial triangle;
- excessive sweating - hyperhidrosis;
- dizziness, unsteadiness of gait;
- flashing "flies", tinnitus.
The pulse rate increases, the filling and tension fall, the tonometer records the decrease in pressure.
Vomiting with blood, like stool changes, are the most characteristic external manifestations of the described traumatic state of the gastrointestinal tract circulatory system.
Vomiting often with clotted blood - "coffee grounds", as it is affected by the hydrochloric acid of the stomach. The appearance of scarlet blood may indicate either bleeding from the esophagus, or profuse (abundant) gastric.
The stool in patients becomes black or very dark in color - melena, due to coagulated and partially digested blood.
In addition to the listed symptoms, there are manifestations of a disease or condition that led to the occurrence of blood loss.

Diagnostic methods
Examination of a patient with suspicion or clear signs of bleeding from the gastrointestinal tract begins with the collection of complaints and anamnesis data.
The provision of a preliminary diagnosis is influenced by a person's intake of medicines, food, and concomitant diseases.
Laboratory tests help assess the degree of blood loss:
- general clinical blood test - the number of corpuscles, the presence of anemia;
- biochemical blood test - assessment of liver and kidney function;
- analysis of feces for occult blood;
- coagulogram - indicators of the blood coagulation system.
The most informative are the instrumental survey methods:


When examining a patient with symptoms of internal bleeding, it is necessary to exclude another pathology: myocardial infarction, ectopic pregnancy in women, nosebleeds and hemoptysis.
Stomach bleeding treatment
Medical tactics, the amount of manipulations depend on the intensity of bleeding and the condition that led to it.
Minor chronic blood loss can be treated conservatively by the specialist who is responsible for the disease that caused this condition.
Profuse vomiting of blood, confusion and loss of consciousness require an immediate emergency call and hospitalization of the patient.
Conservative
- A person is prescribed strict bed rest, cold on the epigastric region (ice pack).
- Applied gastric lavage with cold water, followed by the introduction through an epinephrine tube. This promotes vasospasm and stops bleeding.
- At the same time, the intravenous administration of hemostatic (hemostatic) agents and the infusion of solutions to maintain the volume of circulating blood are started.
- Iron supplements are prescribed to correct anemia.
- In case of massive blood loss, transfusion of blood components is used - fresh frozen plasma, erythrocyte mass.
- Symptomatic treatment is carried out according to indications.

Endoscopic
A favorable method of minimally invasive intervention is endoscopic manipulations. They can serve as a diagnostic procedure and at the same time provide a therapeutic effect.
- When conducting FEGDS and detecting a bleeding ulcer, the latter is injected with solutions of adrenaline or norepinephrine.
- Small damaged areas of the gastric mucosa are cauterized using laser or electrocoagulation.
- More extensive lesions are stitched with surgical sutures or metal clips.

Such manipulations are more easily tolerated by patients, prevent additional blood loss during open operations, but can only be used for minor bleeding.
Surgical

The surgeon chooses an open or laparoscopic approach based on the goals of the operation and the general condition of the patient.
After undergoing surgical treatment, the patient is prescribed a sparing diet, which is gradually expanded.
First aid
If symptoms of gastrointestinal bleeding appear, emergency medical attention is required. It should be borne in mind that with latent blood loss in the gastrointestinal tract, pain in the stomach area does not occur in 90% of cases.
Before the arrival of the ambulance team, the following steps should be taken to alleviate the patient's condition:
- Lay the patient back on a hard or relatively hard surface. When the patient is on the floor, leave it in place, do not move it to the bed.
- When vomiting, control the turn of the head to the side to prevent flooding with vomit.
- Provide cold to the stomach area (ice bladder or, as a handy tool, frozen food, a bottle of cold water). When using ice or frozen food, control the temperature of the refrigerated area to prevent frostbite.
- Absolutely exclude food and liquid intake. In case of an overwhelming thirst, offer an ice cube
- If you have a tonometer, check the pressure readings. Drop in blood pressure below 100 mm Hg. Art may indicate the transition of blood loss from satisfactory to a more severe phase, requiring initial infusion therapy.
Upon arrival, the ambulance should inform about the symptoms manifested, about the blood pressure indications and provide a list of medications that the patient took to control for the presence of anticoagulants and non-steroidal anti-inflammatory drugs prescribed for the treatment of joints.
If necessary, a team of doctors on the spot will perform all the necessary manipulations to stabilize the patient's condition and transport him in a horizontal position to a medical institution, where all the necessary assistance will be provided, corresponding to the patient's condition and preliminary diagnosis.
Complications of gastric bleeding
Excessive bleeding in the stomach can disrupt the functioning of the entire body as a whole.
Common complications include:
- the development of hemorrhagic shock;
- severe anemia;
- acute renal failure;
- multiple organ failure.
Timely seeking medical help can prevent the development of complications. Delay in some cases costs the patient's life.
Prognosis for bleeding from the gastrointestinal tract
The prognosis is determined by the amount of blood loss and the causes of this condition.
- With minor changes and correction of the underlying disease, the prognosis is favorable.
- Abundant blood flow, malignant process have an unfavorable prognosis.
There is only one prevention of gastric bleeding: adequate treatment of the underlying disease and adherence to the recommendations of the attending physician.
Gastrointestinal bleeding - is the outflow of blood from damaged vessels into the cavity of the organs that make up the digestive system. The main risk group for this disorder is older people - from forty-five to sixty years, but it is sometimes diagnosed in children. It is noteworthy that it occurs several times more often in men than in women.
- Etiology
- Classification
- Symptoms
- Diagnostics
- Treatment
- Complications
- Prophylaxis
More than a hundred diseases are known against which such a symptom can develop. These can be gastrointestinal pathologies, various damage to blood vessels, a wide range of blood ailments or portal hypertension.
The nature of the manifestation of the symptoms of the clinical picture directly depends on the degree and type of hemorrhage. The most specific manifestations can be considered the appearance of blood impurities in the vomit and feces, pallor and weakness, as well as severe dizziness and fainting.
The search for a focus of hemorrhage in the gastrointestinal tract is carried out by performing a wide range of instrumental diagnostic methods. To stop GCC, conservative methods or surgery will be required.
Why is there blood from the stomach
Bleeding in the intestines, stomach, or other digestive organs can develop for the following reasons:
The most common causes of gastrointestinal bleeding are duodenal and gastric ulcers. They account for up to 35% of all bleeding from the gastrointestinal tract. Risk factors for the development of peptic ulcer diseases are frequent stress, drinking and smoking.
Important information: How to stop bleeding in a cut (bleeding wounds) and first aid for injuries and bleeding
In children, the most common causes of bleeding are volvulus (for infants) and intestinal polyposis (for preschoolers).
Some causes of intestinal bleeding (for example, hemorrhoids, anal fissures or polyps) provoke only scant spotting or small amounts of blood in the stool. With ulcers, vascular pathologies, tumors and ruptures of the walls of the gastrointestinal tract, blood flows abundantly, mixing with secretions (vomiting, feces) in an altered or unchanged form.
Diagnostic methods

With regard to the differential diagnosis of gastrointestinal bleeding, it offers a complete examination, which begins with anamnesis, assessment of feces and vomit, and performing rectal digital examination. The color of the skin must be taken into account. The abdominal area is gently palpated in order to avoid strengthening the GIQ. It is necessary to review the coagulogram, determine the level of urea and creatine, kidney test.
X-ray methods are useful:
- irrigoscopy;
- celiacography;
- X-ray and angiography.
The most effective and accurate diagnostic method is endoscopy (EGD, gastroscopy and colonoscopy, as well as esophagoscopy). These analyzes will help to establish the presence of a surface defect on the mucous membrane, as well as the source of the fatty tissue.
Classification
Bleeding from the digestive tract is divided into groups depending on the etiology, source of hemorrhage and severity. According to the etiology of bleeding, they are divided:
- on caused by diseases of the gastrointestinal tract (ulcerative and non-ulcer genesis);
- on provoked by impaired blood circulation in the portal vein (portal hypertension);
- for bleeding in vascular diseases;
- on the hematopoietic system caused by pathologies, incl. hemorrhagic diathesis.
In accordance with the classification of bleeding by localization, the following types of this disorder are distinguished:
- bleeding from the upper digestive tract (stomach, esophagus, duodenum 12);
- bleeding from the lower digestive organs (small and large intestine, rectum, hemorrhoids).

Discharge of blood from the upper gastrointestinal tract develops most often. Esophageal, duodenal and gastric bleeding is diagnosed in 8-9 out of 10 patients with bleeding in the digestive tract.
Classification of bleeding by severity
| The severity of the pathology | Decreased circulating blood volume | External manifestations | Systolic blood pressure and pulse rate | Blood indicators |
| Easy | Less than 20% | The patient's condition is satisfactory: the patient has normal urine output (diuresis), slight weakness and dizziness are possible. The patient is awake. | BP - 110 mm Hg Heart rate - no more than 80 bpm | The concentration of erythrocytes is above 3.5 * 1012, the hemoglobin level is more than 100 g / l, the hematocrit is at least 30%. |
| Average | 20-30% | The patient's skin turns pale, severe sweating (cold sweat) is observed, and urine output is moderately reduced. The patient is conscious. | BP - 100-110 mm Hg Heart rate - 80-100 bpm | The concentration of erythrocytes is above 2.5 * 1012, the hemoglobin level is 80-100 g / l, the hematocrit is 25-30%. |
| Heavy | Over 30% | The patient's condition is serious: he has a breakdown, dizziness, severe muscle weakness, severe pallor of the skin, sweating, a decrease in the volume of urine excreted (until complete anuria). The patient's reactions are inhibited, loss of consciousness may be noted. | BP is below 100 mm Hg. Heart rate - more than 100 bpm | The concentration of erythrocytes is below 2.5 * 1012, the hemoglobin level is less than 80 g / l, the hematocrit is less than 25%. |
Some experts also identify the fourth, most severe stage of bleeding. It is characterized by complete loss of consciousness in the patient and the development of a coma.
Massive internal bleeding accompanied by severe blood loss is called profuse.
Additionally, bleeding in the gastrointestinal tract can be classified according to the following criteria:
- duration of bleeding (acute or chronic bleeding);
- the presence of external manifestations of pathology (latent or explicit);
- the frequency and number of cases of blood loss (single or repeated, recurrent).
Intestinal bleeding treatment
After the patient is transported to the hospital, procedures are started. If the loss of biological fluid is significant, then drip administration of plasma or blood is prescribed.
Transfusion volumes:
- Plasma: 50-10 ml, rarely 400 ml.
- Blood: 90-150 ml.
- If the bleeding is profuse: 300-1000 ml.
In addition to drip transfusion, intramuscular injection of blood protein is used, an indication for such procedures is arterial hypertension. With a high level of blood pressure, blood transfusion in a drip manner is impractical.
- the patient needs complete rest;
- compliance with bed rest.
The patient should be in bed, not experiencing any emotional or physical stress that could worsen his condition.
The introduction of homeostatic drugs that can stop or slow down the loss of biological fluid is also practiced:
- Atropine sulfate.
- Benzohexonium solution.
- Rutin, Vikasol.
A solution of Benzohexonium is administered only if the level of blood pressure is not lowered, it helps to reduce intestinal motility, reduce vascular tone, and stop blood loss.
Along with medicines, a person is allowed to swallow a hemostatic sponge, crushed into pieces.
If blood pressure has dropped sharply, drugs are used to increase its level: Caffeine, Cordiamine. If the pressure is below 50 mm, then the blood transfusion is stopped until the pressure level has stabilized.
What are the signs and symptoms
Early symptoms of gastrointestinal bleeding include:
- general weakness, weakness;
- dizziness, fainting, confusion, and loss of consciousness;
- tinnitus, flickering of flies in the eyes;
- nausea, vomiting;
- discoloration of gastric and intestinal secretions (vomiting and feces);
- sweating;
- intense thirst;
- increased heart rate;
- pallor of the skin, cyanosis of the lips, blue discoloration and decreased temperature of the fingertips.

The severity of the symptoms of pathology depends on the intensity of bleeding, BCC and the amount of blood lost. Due to the larger initial volume of circulating blood, bleeding symptoms in adults can manifest later and less brightly than in children. Even minor blood loss in a young child may require immediate resuscitation.
Symptoms of internal bleeding in the stomach often appear simultaneously with signs of massive blood loss and a decrease in circulating blood volume. Against the background of manifestations of blood loss, pain in the affected gastrointestinal tract, an increase in the volume of the abdomen due to the accumulation of fluid (ascites), fever caused by intoxication, weight loss, a sharp change or loss of taste, and other pathological phenomena indicating the cause of the gastrointestinal tract can be observed.
The main symptom of gastric bleeding is bloody vomiting, the nature of which may indicate the cause of the pathology and the duration of the bleeding.
Vomiting with various pathologies of the upper gastrointestinal tract, which lead to blood loss:
"Coffee grounds" is a product of the treatment of blood from the stomach with hydrochloric acid.

With ulcerative lesions during vomiting, stomach pains decrease. Bleeding is not accompanied by irritation of the peritoneum and muscle tension in the anterior abdominal wall. With massive blood loss and stomach cancer, the color of the stool also changes.
Repeated vomiting with blood 1-2 hours after the first episode indicates the continuation of bleeding, and vomiting after 4-6 hours indicates its relapse.
With gastric bleeding, the symptoms of blood loss in most cases are more pronounced than with bleeding in the intestine. This is due to the fact that frequent causes of damage to the walls of the small, colon and rectum are hemorrhoidal trauma, polyposis and small cracks in the mucosa. They can provoke prolonged, but insignificant blood loss, which is accompanied by a slight decrease in the concentration of hemoglobin and the development of compensatory tachycardia while maintaining normal blood pressure and the patient's well-being.
Symptoms of intestinal bleeding accompanied by massive blood loss may include:
- black feces;
- discharge of melena (loose tarry stools with a strong unpleasant odor);
- weakness, loss of consciousness, pallor of the skin and other manifestations of acute blood loss.
Visual changes in the color and structure of feces are visible only with blood loss of more than 100 ml / day and damage to the rectum and colon (cracks, polyps, bleeding hemorrhoids). With a single outflow of blood (with stomach ulcers and pathologies of the lower digestive tract), blood is excreted in the stool unchanged. With prolonged massive bleeding, a tarry stool (dark feces with small clots) is released a few hours after its onset.
The nature of stool changes in various intestinal pathologies:
In the chronic course of the pathology, symptoms of anemia may occur:
- weakness, fatigue;
- decreased performance;
- frequent dizziness;
- inflammation of the mouth and tongue;
- pallor of the mucous membranes and skin.
Types of internal bleeding of the digestive system
Intragastric bleeding may occur once and no longer disturb the person, or repeat from time to time. In the second case, we can talk about a relapsing state. In this case, the patient needs a thorough examination, which will help to identify the whole complex of reasons that each time lead to blood loss.

Acute develops suddenly and rapidly, leads to the loss of large volumes of blood and a sharp deterioration in the general condition. The person needs urgent medical attention as there is a risk of losing a large volume of blood. Signs include vomiting of scarlet blood, confusion, low blood pressure (the top reading is below 100), and loss of consciousness.
Chronic symptoms can last for days or even weeks. For the patient, it often goes unnoticed, but iron deficiency anemia develops over time. Do not hope that after a while this state will pass by itself: examination and medical care are necessary to stabilize the condition.
Depending on the amount of blood loss, it can be:
- Light - practically does not appear. A person may notice a small amount of blood in feces or vomit. Small vessels are usually affected and blood loss is negligible.
- Secondary mild dizziness and a slight decrease in blood pressure.
- Severe, in which a person can lose consciousness, not react to the environment.
A patient with intestinal bleeding should be provided with rest and medical advice. The more severe the condition, the faster the help of doctors is needed. If the state of health is satisfactory, it is still necessary to consult a therapist or gastroenterologist.
Diagnostics
Elucidation of the cause of gastrointestinal bleeding syndrome requires a thorough clinical examination, laboratory tests, and the use of hardware and instrumental diagnostic methods.
Clinical examination
With the initial diagnosis of internal bleeding in the stomach or intestines, a clinical examination of the patient is carried out, during which the following data are analyzed:
- patient history;
- list of medications taken;
- the color and consistency of the discharge;
- skin color (pallor, yellowness);
- the presence of vascular "asterisks", hemorrhagic manifestations and other vascular pathologies on the skin.

If there is a suspicion of intestinal or gastric bleeding, palpation of the painful abdomen and rectal examination are performed with caution. Inaccurate procedure can significantly increase blood loss.
Laboratory research
Laboratory tests that are performed for bleeding in the stomach, esophagus and lower gastrointestinal tract include:
- general blood analysis;
- blood biochemistry (liver and kidney tests, markers of inflammatory processes, etc.);
- coagulogram;
- coprogram;
- analysis of antibodies to double-stranded DNA, etc.
Instrumental methods
The most informative hardware diagnostic methods that are used when intragastric and intraintestinal hemorrhage is suspected are:
- X-ray examination of the esophagus and stomach;
- celiacography;
- MR-angiography of the gastrointestinal tract vessels;
- static and dynamic scintigraphy of the digestive tract;
- CT scan of the abdominal organs;
- X-ray of the nasopharynx, bronchi and lungs.

Most rapidly bleeding in the stomach can be diagnosed with upper gastrointestinal endoscopy. For pathologies of the lower parts of the tract, irrigoscopy, sigmoidoscopy and colonoscopy are used.
If it is impossible to establish the source of hemorrhage using endoscopy and hardware methods, diagnostic laparotomy is performed.
The factors for the development of the disease are multiple. It is necessary to identify the provocateur as quickly as possible. Even if it is possible to completely eliminate the pathological process, no one can guarantee that a relapse will not happen. It will most likely be so.
Among the main factors:
Stomach ulcer
According to studies prior to 2010, this point was considered a key point in the etiology. As it turned out later, not everything is so simple. The risks are really growing, which is quite obvious.
The reason for gastric bleeding is as follows: the normal integrity of the mucous membrane is disrupted, the tissues of the organ are richly supplied with blood, therefore any destructive, structural changes with a high probability will lead to a violation of the state of the local vascular (vascular) network.

However, despite the possibility of high-quality treatment and breakthroughs in medicine, the statistics on gastric bleeding do not change. Doctors assume that there is a group of disorders. Among which the ulcer plays an important role, but this is not the only and not the exclusive cause of hemorrhage in the stomach.
Cancer violations
Tumors. Often we are talking about completely benign structures. These are the so-called polyps. In fact, their good quality in a broad sense is rather arbitrary.
They grow quite deep into the tissue, eventually causing disruption of the local circulatory network. Also, do not forget about the possibility of cancerous transformation.

Malignant tumors cause bleeding in the gastrointestinal tract almost from the first stages. But critically acute conditions are observed closer to the final phase of the disease. When active disintegration and infiltrative germination begins through all the walls and layers of the stomach.
Digestive tract injuries
Observed as a result of the influence of a mechanical factor. Mostly. We are talking about the consumption of inedible objects, sharp objects with perforation of the wall of a hollow organ, also about impact, the effect of direct kinetic force. For example, during an accident, fighting, when falling from a great height.
Against the background of this disorder, direct ruptures of the stomach are possible, which leads to the outflow of blood into the cavity of the organ or into the peritoneum.
Invasive interventions
Including diagnostic ones. There is an iatrogenic effect. In this case, the doctors are to blame. Medical procedures can provoke problems of this kind, even if they are performed correctly and technically correctly.
The question lies in the individual characteristics of the human body. Medical errors cannot be ruled out, this also occurs.
Liver pathology
Hepatitis, cirrhosis, tumor processes. Mainly in sub- and decompensation. In this organ, a number of coagulation factors are produced. Without normal functional activity, there is no way to ensure adequate coagulation. Therefore, violations begin. The more significant the problem, the more dangerous the pathological processes themselves.
Disorders from the hematopoietic system itself
From hemophilia to others. The entire list of diagnoses located in the classifier in the appropriate section, one way or another, can provoke gastric bleeding.
Hypocoagulation
The generalized name of the processes during which there is a decrease in coagulation. Usually this is not an independent diagnosis, but just a syndrome, a clinical finding. Read more about the causes of poor blood clotting in this article.

These are the main causes of intragastric bleeding. There are others. The list is incomplete.
How to stop bleeding
Stopping bleeding should be carried out by doctors of a medical institution or emergency medical team. Even before providing emergency care, it is necessary to call an ambulance, outlining the patient's condition and the nature of the discharge.
The algorithm for providing emergency first aid if bleeding is suspected includes the following actions:
- lay the patient on his back, raising his legs using rolled clothes or a pillow;
- do not give the victim to drink and eat;
- put a compress of ice wrapped in a cloth on the painful area;
- during the provision of first aid, monitor the nature of breathing and heart rate;
- in case of loss of consciousness, bring the patient to life with a cotton swab dipped in ammonia;
- when waiting for an ambulance for a long time, carry the patient on a stretcher towards the medical team.

During the provision of emergency care for gastric bleeding, it is forbidden to wash the stomach. If an intestinal pathology is suspected, an enema should not be given to the patient.
An attempt to stop the blood without the help of doctors can lead to the death of the patient.
Emergency Stomach Bleeding
What is the emergency treatment for stomach bleeding? All necessary actions are listed below:
- Providing bed rest, which helps to reduce the rate of bleeding.
- Setting up a cold compress (the algorithm will be discussed below).
- Washing the stomach with ice water, the essence lies in the spasm of the bleeding vessels and the subsequent stop or slowdown of the blood flow.
- Prescribing epinephrine or norepinephrine medications via a gastric tube. This group of hormones refers to stress factors that cause compensatory narrowing of the vascular lumen.
- Replenishment of reserves of the total volume of circulating blood (BCC) by introducing hemostatic solutions intravenously.
- Use as a replacement for lost donor blood, blood substitutes and frozen plasma.
Other therapy is carried out when indicated.
How to treat
With gastrointestinal bleeding, treatment is aimed at stopping it, eliminating the root cause of the pathology, restoring hemostasis of the body and normal blood volume.
The danger for the patient is not only the loss of red blood cells that carry oxygen, but also a sharp decrease in the BCC, which leads to massive thrombosis of small vessels and the development of DIC.
Conservative treatment
Conservative treatment of gastric bleeding and intestinal blood loss is performed as an adjunct to surgery. As the main method of therapy, it is used for the following indications:
- hemorrhagic syndromes;
- cardiovascular diseases;
- inoperable malignant tumors;
- congenital pathologies of the hematopoietic system.
In therapy, hemostatic agents, cytostatics, anti-inflammatory and other drugs can be used.

If a large volume of blood is lost, the patient is prescribed droppers with saline solutions and transfusions of blood components.
Surgery
If there is a suspicion of bleeding in the gastrointestinal tract, the patient is taken to the surgical department of clinics, where diagnostics and determination of therapy tactics take place.
Depending on the diagnosis, the patient can undergo the following operations:
- endoscopic sclerosis, electrocoagulation and ligation of dilated vessels of the intestine, esophagus, etc.;
- suturing of the ulcer and partial resection of the stomach;
- suturing duodenal ulcer;
- subtotal large intestine resection with stoma.
Diet
The tactics of treatment with diet therapy depends on the underlying disease. With pathologies of the stomach, the patient is assigned a table No. 1, No. 1a (immediately after stopping the bleeding), No. 1b or No. 2. For bowel diseases, diet no. 3 or no. 4 is recommended.
If the discharge of blood is a complication of hepatic pathology, the patient is assigned table number 5 and its variations.
Prophylaxis
Specific preventive measures for such a disorder have not been developed; in order to avoid problems with hemorrhages in the gastrointestinal tract, it is necessary:
- timely treat diseases that can lead to the appearance of such a complication;
- undergo regular examination of an adult and a child by a gastroenterologist.
The prognosis directly depends on the predisposing factors, the degree of blood loss, the severity of the accompanying ailments and the age category of the patient. The risk of complications and mortality is always extremely high.
How to prevent the phenomenon
To prevent the development of this dangerous pathology, it is necessary to undergo regular medical examinations, follow the rules for taking medications and lead a healthy lifestyle.
Contacting a gastroenterologist at the first manifestations of ulcerative and vascular diseases (malaise, nausea, stomach pains, etc.) increases the likelihood of a favorable prognosis for the effectiveness of therapy.
To track intestinal bleeding in the early stages, it is recommended to regularly take a fecal occult blood test.
Cold compress
A relationship of trust must be established with the patient. He needs to understand the purpose and course of the cold compress. The algorithm of actions performed with his consent is as follows:

Recovery period: lifestyle and diet
After undergoing a course of drug treatment, the specialist strongly recommends that the patient change his lifestyle and diet. You should exclude intense physical activity for at least 4 weeks, avoid hypothermia, stress, do not go to saunas and baths, and ensure yourself a full night's sleep.

It is worth excluding from the diet:
- fat meat,
- salted and smoked fish,
- canned vegetables, fruits, marinades,
- seasonings,
- alcohol,
- strong coffee,
- soda,
- fast food,
- confectionery, baked goods.
The portions should be small, the food is low-fat, pureed, and the meals should be at least 5 times a day at regular intervals. After 4-6 weeks of adherence to the diet, it is allowed to make it less strict, but only after consulting a doctor.
The patient's menu must include the following products:
- scrambled eggs;
- biscuit biscuits, crackers;
- weak black tea;
- cereals;
- a small amount of potatoes;
- steamed poultry, fish;
- mashed soups;
- a little butter, dairy products.
If the patient has undergone surgery to suture the stomach, the first day after the manipulation, he does not use anything. On the second day and over the next week, chicken breast broth without skin, as well as dried fruit compote, are poured into his nasal probe. The daily rate is 1 liter of each of these liquids. On the 7-10th day, they are allowed to start gradually taking food: mashed potatoes without butter, soft-boiled egg, grated soup without frying.
The patient's lifestyle after surgery plays an important role. The first 10 days, it is strictly forbidden to get up, after the specialist removes one or all of the tubes, the patient is allowed to get up for a short time. The recovery period lasts at least 6 weeks. Recommendations are similar to those given to patients after undergoing conservative treatment.
Indications for surgical treatment
Acute gastric bleeding is an indication for surgery when:
- lack of positive results from previously conducted conservative and endoscopic measures;
- unstable condition of the patient or severe, which may be complicated in the near future (for example, ischemic disease or stroke);
- repeated bleeding.

First aid
With severe and prolonged bleeding, the patient may experience blue lips. Often, the patient has a feeling of lack of air. Vision may be severely impaired. The human condition is deteriorating dramatically. Such symptoms clearly indicate acute gastric bleeding. An "emergency" must be called immediately. Any time wasting is fraught with serious consequences. Statistics show that more than 17% of patients die from gastric blood loss.
What to do before the arrival of the medical team? First aid for gastric bleeding is to provide the patient with complete rest. It is recommended to lay the patient horizontally. It is strictly forbidden to give him food or water. If possible, put cold on the stomach, in the upper region. It can be a bubble or an ice bag. Doing enemas, rinsing the stomach is impossible in any case!
It is necessary to closely monitor the general condition of the patient. If he loses consciousness, be sure to revive him. For such purposes, use a cotton swab dipped in ammonia.
A. Emergency colonoscopy
B. Emergency sigmoidoscopy
B. Irrigoscopy
D. Plain fluoroscopy of the abdominal organs
E. Control of passage through the gastrointestinal tract of barium administered per os
Features of the course in adults and children
Symptoms of the disease in an adult and a child are almost the same. But in the former, the disease often develops gradually, they do not pay attention to the first signs, therefore complications often develop. In children, GCC is always acute, but due to the rapid restoration of blood vessels and gastric mucosa, symptoms may appear for a short time and disappear. The kid becomes active again, plays and asks for food. You should not postpone the visit to the doctor, even if there were no repeated manifestations during the day.
Rehabilitation
Blood loss entails a change in the structure of the affected tissues, and it takes time for them to heal. The first 2-3 days, nutrients are administered intravenously to the victim and gradually transferred to a standard diet in compliance with a strict diet.
The lesions heal for at least six months, and all this time the patient's diet should be given the utmost attention. After 6 months, the patient is re-examined by a gastroenterologist.
Rehabilitation measures after surgery
- Day one - you can move your arms and legs.
- Day two - the beginning of the introduction of breathing exercises.
- Day three - you can try to get on your feet.
- Day eight - postoperative stitches are removed.
- Day fourteen - discharge from the department with recommendations to limit physical activity for a month and the need to perform a set of physiotherapy exercises.

The need for surgical intervention
Surgical treatment of patients can be divided into 2 ways - active and expectant tactics. In the first case, doctors perform surgery at the level of hemorrhage.
Expectant treatment tactics include stopping the flow of blood using conservative means. Then the surgeons perform a planned operation.

Surgical treatment is carried out in the diagnosis of profuse bleeding, ulcers in the projection of the great vessels, with an unfavorable endoscopic examination.
The preparation of the patient takes about 2 hours and depends on the intensity of the hemorrhage. To stop gastroduodenal bleeding, the use of endotracheal anesthesia is appropriate.
If the patient does not have an ulcer or other pathological lesions of the walls of the stomach, then a longitudinal gastrotomy can be performed.
All bleeding vessels are sutured, ligated and diathermocoagulated.
The duration of the operation depends on the patient's condition and possible complications. If patients are in a difficult situation, then palliative surgery is urgently needed.
Doctors carefully suture the bleeding vessels and perform a wedge-shaped excision of the ulcer. Stitching of the stomach walls and placement of the serous-muscular ganglion may be required.
Possible complications
The main complications are:
- the appearance of hemorrhagic shock from blood loss;
- the development of acute iron deficiency anemia;
- acute hepatic and renal failure.

A life-threatening situation is the development of multiple organ failure, when the function of several vital organs and systems suffers. In such a situation, patients need resuscitation measures to save life. Any attempts at self-treatment or lack of timely hospitalization often lead to the death of the patient.
