Anatomy of the elbow joint
The elbow joint is formed by the distal part humerus and the proximal parts of the radius and ulna. It is very important that each bone clearly and evenly forms the elbow joint so that the load during movements is distributed evenly and there is no pathological shift of the load from one edge to the other.
Short radius syndrome disrupts the balance of the joint. If during the active growth of the puppy (the main growth of the dog large breed takes 4-8 months) damage to the growth zone of the radius occurs, this can lead to early post-traumatic closure of the metaphysis and cessation of the formation of the radial bone in length, that is, its elongation. This in turn leads to a deformation of the articular surface of the elbow joint, when the humerus begins to touch and exert full pressure only on the articular surface of the ulna. This is clearly visible in the photo (shown by two arrows). Also, such uneven growth of the forearm bones may be associated with a breed predisposition or other unidentified reasons.
The humerus puts all the pressure on the ulna, which leads to destruction of the underlying tissues (cartilage and bone) and even fragmentation of areas of bone on the medial and lateral sides.
Symptoms of a shortened radius
Most cases occur in dogs under one year of age. The most susceptible breeds are: Bernese Mountain Dog, retrievers, mastiffs and other large dogs. The disease manifests itself as lameness in the affected forelimb. There may also be some pronation (rotation) of the forearm to reduce pain in the joint. Palpation can reveal swelling in the joint due to the accumulation of inflammatory synovium. The elbow joint is limited in movement (flexion-extension).
Diagnosis is quite simple. The radiograph shows shortening of the radius relative to the ulna. The radius extends beyond the joint (see below). CT can be used to diagnose secondary lesions such as fragmentation of the coronoid process elbow joint
Treatment is only surgical. It involves removing a segment of the ulna bone below the elbow joint. The amount of bone tissue that is removed is inversely proportional to the age of the dogs. In other words, if the dog is young (ie around 5 months), then a significantly wider segment must be removed from the ulna compared to a dog that is no longer growing (around 10 to 12 months). You can also wire the ends of the ulna to correct the relationship between the components of the elbow joint immediately after surgery. The space between the ends of the ulna heals over time, but this process can take up to 3 months if the defect is large. This operation, dynamic osteotomy of the ulna, is indicated for growing dogs.
A more complex form of treatment involves lengthening the radius itself, but this method is used for dogs that have stopped forming.
If necessary, fragmented areas can be removed arthroscopically or on an open joint, but this is not the primary therapy.
 Preoperative radiograph shows a shortened radius and a joint defect of approximately 6 mm of discrepancy Preoperative radiograph shows a shortened radius and a joint defect of approximately 6 mm of discrepancy |
 X-ray before surgery in direct projection X-ray before surgery in direct projection |
 An x-ray immediately after surgery shows the comparison of the components of the elbow joint, the formation of congruence. IN in this case 1.5 cm of bone tissue was removed. An x-ray immediately after surgery shows the comparison of the components of the elbow joint, the formation of congruence. IN in this case 1.5 cm of bone tissue was removed. |
 X-ray after surgery in direct projection X-ray after surgery in direct projection |
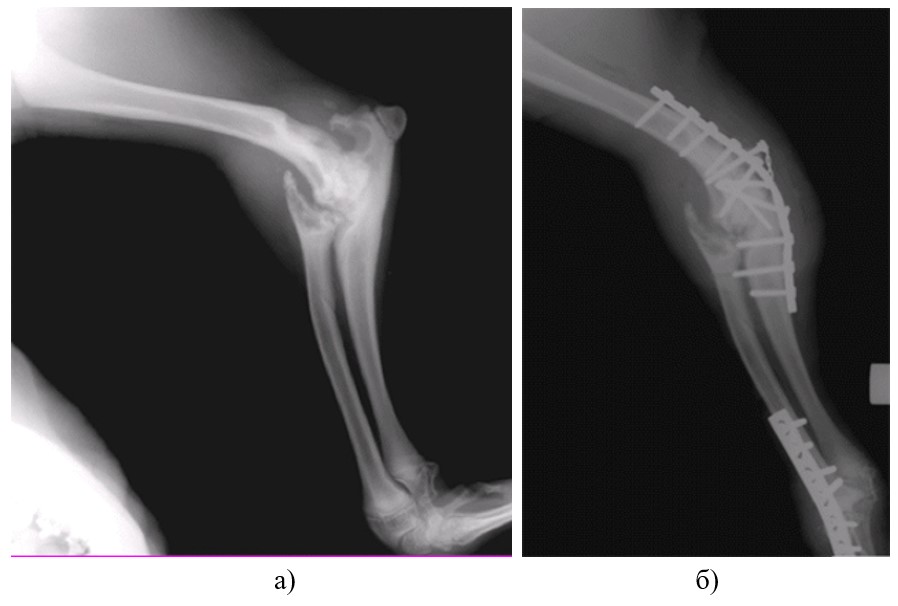
For 15 years the clinic has been treating hallux valgus deformity thoracic limb in dogs. To date, a unified treatment strategy for this pathology has been developed. In animals during the period of intensive growth from 4.5 to 9 months, the distal growth zone of the radius is blocked with metal staples with a simultaneous segmental osteotomy of the ulnar diaphysis (Fig. 1). This makes it possible to level out limb deformity in 70-80% of animals and avoid more complex surgery.
Fig. 1 X-ray of the bones of the forearm in frontal and lateral projection. Blocking the distal growth zone of the radius with medial surface(a, b). X-ray of the forearm bones in frontal and lateral projections 1 month after surgery. Leveling angular deformation.
If the deformity persists, then at the end of intensive skeletal growth the animal can undergo a one-step correction of the deformity of the forearm bones by means of a wedge-shaped osteotomy of the radius at the apex of the deformity angle, an oblique osteotomy of the ulna, one-step correction of the axial deformity and fixation of bone fragments in the G.A. apparatus. Ilizarov (Fig. 2). It must be remembered that performing this operation before the end of intensive skeletal growth leads to recurrence of deformation of the forearm bones due to the continuation of uneven bone growth.


Rice. 2. A - Dog with valgus deformity (indicated by the arrow) of the left thoracic limb (carpus valgus). B — Wedge-shaped osteotomy of the radius with simultaneous correction of deformity and fixation in the G.A. apparatus. Ilizarov. B — Stage of the operation: removal of a wedge-shaped fragment of the radius. Animal in the apparatus and after removal of the external fixator (D, E).
- Varus (o-shaped) deformity of the thoracic limbs



Rice. 3. Macro photo. Varus (o-shaped) deformity of the forearm bones in a Staffordshire terrier dog (a). X-ray of the bones of the right thoracic limb in a direct projection - varus deformity (b): 1-line parallel to the articular surface wrist joint; 2-axis of the radius; 3-angle of deformation of the radius. Macro photo (B). Device module G.A. Ilizarov. Thoracic limb with marked landmarks for performing wedge-shaped osteotomy.
- Valgus deformity of the pelvic limbs (genu valgum)
Valgus deformity of the pelvic limbs in dogs is caused by an increase in the neck-diaphyseal angle of the femur, which leads to severe deformation of the femur and tibia, which together gives an X-shaped position of the pelvic limbs. To make this diagnosis, it is necessary to take radiographs of the pelvis in the first position.

Rice. 4. Radiographs of the pelvis in the first position. Increased neck-shaft angle of the right and left hip joints (a). X-shaped deformity of both pelvic limbs (b). Macro photo. X – shaped pelvic limbs (c).
To correct valgus deformity of the pelvic limbs, the animal underwent intertrochanteric osteotomy of the femur and wedge-shaped osteotomy of the tibia. Surgery on the second limb was performed at intervals of 1 month. Special implants were used to fix the fragments. The removal of the plates was not carried out at the request of the owners.

Rice. 5. X-ray of the pelvis in the first position, after performing a staged intertrochanteric osteotomy of the right and left femur and wedge-shaped osteotomy of the right and left tibia (a). Animal 1.5 years after surgery (b).
- Neurogenic contractures and congenital anomalies of the limbs
In some cases, it is impossible to determine the cause of neurogenic joint contracture due to the lack of a medical history. This animal was admitted to the clinic with severe contracture of the wrist and elbow joints, shortening of the right thoracic limb due to the destruction of the proximal growth zone of the radius (Fig. 1a, b). Due to the destruction of the articular surface of the elbow joint and severe contracture of the wrist joint with loss of extensor function (neurogenic nature), the animal underwent arthrodesis of the elbow and wrist joints, which made it possible to achieve correct positioning of the limb.

Rice. 1. Macro photo. Contracture of the wrist and elbow joints, shortening of the right thoracic limb (a, b).

Rice. 6. Radiographs of the right thoracic limb in the lateral projection. Destruction of the articular surface of the elbow joint (a). Arthrodesis of the elbow and wrist joints in a physiologically advantageous position using bone plates(b). Completed arthrodesis of the elbow and wrist joint (c). Macro photo. Leveling the angular deformity of the right thoracic limb (d). However, after the operations, the thoracic limb remains shortened by 5 cm.
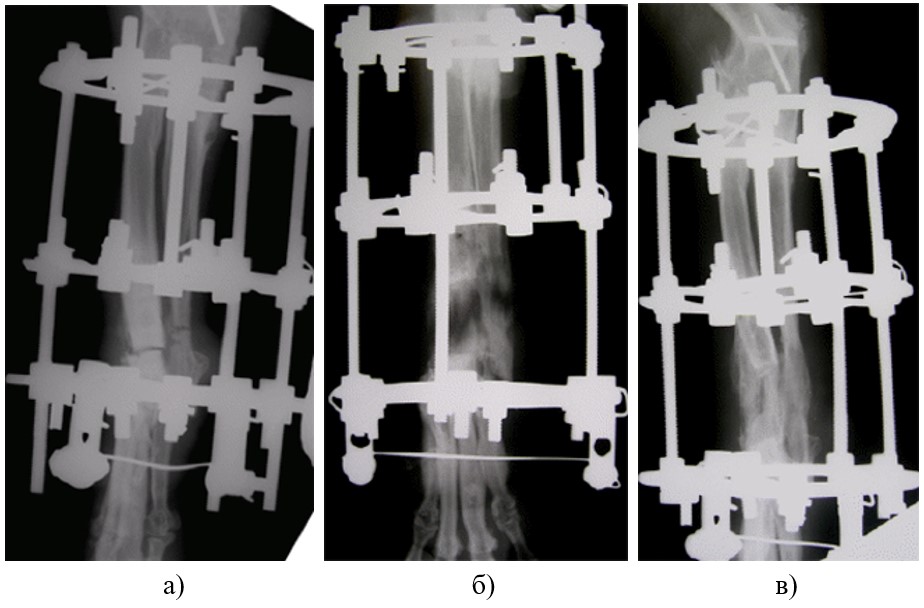

Rice. 7. To lengthen the limb and restore the supporting function, the animal underwent transverse osteotomy of the radial and ulnar bones of the forearm in the apparatus of G.A. Ilizarov (a) and distraction (lengthening) of the bone was performed (b - formation of a growth zone of the regenerate). After the regenerate matured, the animal’s apparatus was removed (c, d).
(!!!) You can compare the photographs of this animal at the beginning and end of the presentation. In our opinion, this is an excellent result, which became a symbiosis of patience, courage, desire to help the animal on the part of the animal owners and the professionalism of the doctors.
- Valgus (x-shaped deformity) of the right tibia.
The animal underwent a wedge-shaped osteotomy of the tibia, with immediate correction of the deformity and fixation of fragments with an LC-DCP plate. Restoring the supporting function of the limb on the first day after surgery.


- 1, 2 — Valgus (x-shaped deformity) of the right pelvic limb.
- 3 - Deformed axis of the tibia and foot of the right pelvic limb.
- 4 — X-ray of the right tibia in a direct projection.
- 5 — View of the animal on the 12th day after surgery. Corrected limb axis.
- 6 — Osteotomy of the tibia, correction of the limb axis, fixation with a plate.
(!!!) I would like to express my gratitude to A.A. Shreiner, N.V. Petrovskaya, and in their person all the employees of the Center for Restorative Traumatology and Orthopedics named after. G.A. Ilizarov, for the opportunity to professionally use the Ilizarov method in the practice of small domestic animals.
(!!!) Thank V.A. Fokin - the person who discovered the technology of osteosynthesis in our country not only for doctors of humanitarian medicine, but also for veterinarians.
Osteotomy is surgery, used in cases where it is necessary to eliminate a defect in bone tissue. Most often, the procedure is performed to restore bone after deformative damage.
Various segments can be operated on, including the bones of the legs and face. Osteotomy can only be performed in a hospital setting; it is not performed in clinics. Unfortunately there is a risk postoperative complications, especially if serious mistakes were made during the rehabilitation period.
The operation can be complex (when treating large leg bones, for example) or simple (mini-osteotomy). The risk of postoperative complications is higher in case of complex technique.
1 What is osteotomy: general description of the operation
Nowadays, almost any problem associated with deformative lesions of bones and joints can be solved without problems. It is to solve such problems that osteotomy is used.
The procedure is intended to eliminate bone defects and the consequences of tissue deformation. With the help of surgery, you can restore the functions of the musculoskeletal system, including through an artificial fracture.
A patient’s limb may be deliberately broken at the level where his deformity is localized. This technique is often used for congenital or acquired pathologies (for example, malunion of a fracture).
Due to its description and method of implementation, osteotomy can scare off most patients. In fact, everything is not as scary as it might seem: the patient does not feel anything during the operation (except perhaps moderate discomfort associated with the work of receptors that record mechanical stress).
The procedure has two types of implementation: through a small incision on skin or by making several holes in the skin. This technique It is used for both children and adult patients of different age groups.
1.1 What is it used for?
The procedure is applicable for the following groups of bones and joints:
- lower and upper jaw;
- pelvic bones, hip joints;
- shin bones, knee joint, metatarsal bone;
- elbow joints, bones upper limbs, including fingers and radius bones;
- it is possible to treat the femur (a rather complex procedure with risks of postoperative complications).
It is important to understand that each group of bones has its own nuances surgical intervention. In addition, different techniques can be used even for the same group of bones, but with different diseases.
For example, treat femur possible using the corrective and restorative method of osteotomy. The first option is suitable in cases where there is an incorrectly healed fracture. The second option is preferable for hip subluxation.
The final choice of technique remains with the attending physician. It is done after a series of diagnostic procedures.
1.2 Indications for testing
There are enough indications for osteotomy a large number of, because besides common diseases(which can affect different joints and bones) there are also specific ones that arise only in a certain group.

Osteotomy is performed for the following pathologies:
- Incorrectly healed fracture of one or another group of bones (in this case, it is possible to carry out an artificial fracture with subsequent normal healing of the bone).
- Ankylosis of the joint in a vicious position.
- Coxarthrosis
- Valgus deformity.
- Consequences of rickets in the form of curvature (deformation) of bones.
- Traumatic deformative lesions.
- Shortening or pathological lengthening of the bone.
- Dislocations and subluxations of bones or joints.
- Birth defects and structural abnormalities of certain bones.
- Varus deformity.
- False joint of the femoral neck.
The operation is often performed for various subtypes of arthritis (for example, psoriatic). The fact is that arthritis can lead to joint or bone deformities. As a rule, this happens only in the most advanced cases, when the disease lasts long enough.
The specificity of the procedure is the cure of deformative lesions as a result of injuries or complications of bones, but not joints. Treatment of complications various types arthritis is only an auxiliary function of osteotomy, which is not used constantly.
1.3 Contraindications
There are a fairly large number of contraindications to the procedure. They cannot be ignored, because in this case the situation can be aggravated, even to the point of disability.
Osteotomy cannot be performed in the following cases:
- during acute onset or exacerbation of rheumatoid arthritis;
- third degree of patellofemoral subtype of arthrosis;
- obesity in a patient of 2-3 degrees ( relative contraindication, in some cases ignored with the permission of the attending physician);
- presence of osteoporosis;
- violations of the regenerative functions of the body, in particular local ones (in terms of bone tissue regeneration);
- infectious pathologies of bone tissue (for example, syphilis or bone tuberculosis) - active or suffered in the recent past;
- arthrosis lesions (degenerative-dystrophic), localized in the collateral parts of the joints.

In addition, surgery cannot be performed if general weakness sick, exhaustion, cachexia, fever (even with minimal elevated temperature). Surgery is also prohibited if a clear diagnosis has not been established: for example, there are deformative bone lesions, but it is not known what caused them. First, a full diagnosis is made - then a decision is made to perform an operation.
2 Types of osteotomy
The operation has two types of conduct: closed and open method.
In a closed procedure, the operation is performed through a small (endoscopic) incision in the skin. The incision size usually does not exceed 2 centimeters. During a closed osteotomy, the doctor literally crosses the bones blindly using a special chisel. This is a difficult and dangerous technique, since incorrect actions by a specialist can lead to a number of serious complications.
Open osteotomy is used much more often, including due to lower risks of serious complications. Here the doctor is no longer working blindly: there is the possibility of full visualization of the operated tissues. The incision on the skin for this technique is much larger and is up to 12 centimeters in length.
Osteotomy is also divided into several subtypes:
- Linear subtype (transverse or oblique). The diseased bone is cut in such a way that it is then smoothed using a graft (plates). In dental implantology, intercortical osteotomy is performed to eliminate jaw defects.
- Wedge-shaped subtype (akin, Akin). During the procedure, part of the bone tissue is removed from the patient, due to which the remaining intact bone is subsequently aligned.
- Z-shaped subtype. Used to treat hallux valgus. During the procedure, the doctor removes overgrown tissue.
- Angular subtype. Bone tissue are carefully cut at certain angles on both sides, due to which it is possible to put them in the required position.
3 How is the operation performed?
There is no universal method for performing osteotomy: each case (disease) uses its own technique.
For example, during corrective surgery on the pelvic bones, the ilium is cut in the area above acetabulum. Next, the pelvic joint is displaced to create an artificial “shield” over the articular head. The procedure is performed under endotracheal anesthesia (the safest option in this case).

Operation knee joints usually performed to treat deforming arthrosis. The tibia is transected, which leads to improved metabolism in the joint tissue by eliminating stagnation of venous circulation.
The feet are usually treated for hallux valgus. To do this, the doctor makes an incision at the end of the bone adjacent to the thumb, followed by placing it closer to the inside of the foot. As a result, it is possible to eliminate the displacement, but sometimes it is necessary to remove part of the overgrown bone tissue.
Sometimes doctors use some tricks when operating on non-specific cases of diseases. That is, right during the operation, the standard tactics of action may change. As a rule, this is only in the best possible way affects the patient's recovery.
Whatever specific procedure is performed, there is always a non-zero chance of complications after the operation. Often complications are caused by improperly carried out rehabilitation stage.
3.1 Where is it carried out and how much does it cost?
So complex surgical procedures carried out only in large public hospitals or private clinics. It is advisable to contact the relevant medical centers, dealing exclusively with diseases of the musculoskeletal system.
The cost depends on the type of surgery. For example, a corrective osteotomy costs around 50,000 rubles. average cost procedures, regardless of its type, range from 60-65 thousand rubles.
3.2 Dressing after osteotomy (video)
3.3 Rehabilitation after osteotomy
Restoring the function of the operated bone is at least 50% of the success of the entire treatment.
It is important to understand that in most cases, the bone will no longer be functionally the same as it was before the disease and surgery. However, it is possible that the functionality will be restored in such a way that there will not be much difference (in terms of sensations).
How exactly rehabilitation should be carried out after an osteotomy depends on which method of operation was performed and on what area.
There are general rules:
- For the first time after the procedure, complete rest of the area that was operated on is required. There should not be any load, even minimal.
- Later the patient is prescribed minimal physical activity to restore bone functionality. A dosed load triggers the acceleration of regeneration of operated tissues. The decision about when and how to load the operated part of the body should be made only by the attending physician.
- Medical corsets, orthopedic insoles and other tools can be used to reduce the load on the bones.
- Medications (anti-inflammatory, regenerative) must be prescribed. Painkillers and muscle relaxants may be used as needed.
Recovery from an osteotomy may take several months. It is very important to follow all the doctor’s instructions: improper rehabilitation can not only ruin the effect of treatment, but also make it worse than it was before the operation.
Possible treatment options(Continued. Started in No. 3.2012)
Considering the proposed methods, for the treatment of end-stage MVO disease, we prefer subtotal osteotomy of the coronoid process (Fig. 2), in which the pyramidal part of the medial coronoid process, which forms the articular part distal to the level of the radial notch, is removed. Surgical intervention involves blunt separation of the flexor carpi radialis/pronator teres and flexor digitorum superficialis/deep muscles caudal to the medial collateral ligament to gain access, and then an incision is made on the medial surface of the joint capsule proximal to the fan-shaped attachment zone of the biceps brachii muscle on the medial aspect of the coronoid process. To facilitate access to the medial part of the joint, self-retaining retractors are used, which are secured caudal to the medial collateral ligament. We used a pneumatic pendulum saw for the osteotomy, 28 but similar effectiveness can be achieved using an osteotome or shaver.
The caudolateral boundary of the osteotomy was the junction of the radial notch and a point 1–2 mm distal to the sagittal edge of the ulnar notch. Microcracks of the subchondral bone extended to the border of this osteotomy line, 6 but the osteotomy zone included the entire area of visible pathology of the cartilage and subchondral bone, determined histomorphometrically. 6 Our initial concerns about elbow instability (due to disruption of the ulnar collateral ligament) were not confirmed.
Subtotal osteotomy of the coronoid process in 263 dogs (437 elbows) achieved permanent and long-term (follow-up in some cases lasted 4-5 years) elimination of lameness with a low percentage of complications after surgical treatment. 28 Other surgical methods local treatment MVO pathologies include removal of loose fragments, varying degrees of clearance from destroyed material, curettage or excision of a portion of the MVO with visible damage, by arthroscopy or arthrotomy. 4,14,17,40–44
Although histological findings suggest that this approach leaves a significant portion of damaged subchondral bone in place 6 , we are not aware of any clinical researches, which would clearly demonstrate the superiority of more aggressive arthroplasty (eg, subtotal coronoid osteotomy) over less aggressive approaches in terms of outcome. A cohort comparative study is needed. If possible reasons MVO pathologies are dynamic joint incongruence or abnormal dynamic loading, corrective osteotomy should probably be considered; however without good understanding mechanics it is unclear which configuration for osteotomy will give best effect. In our experience, ulnar osteotomy results in lameness lasting several weeks. In addition, the severity of lameness is usually greater than before surgery or only after intra-articular intervention. This result eliminates any possible benefit, By at least, in our experience; the long-term outcome is equivalent to that of dogs with MVO pathology without significant changes in the humeral condyle. However, if there is damage due to abrasion in the area of the medial part of the humeral condyle or if there is obvious incongruence of the humerus and ulna visible on CT or arthroscopy, ulnar osteotomy is warranted, as discussed below. We do not see the need for ulnar osteotomy unless the radius and ulna are clearly incongruent >4 mm.
To determine whether TSDM reduces contact pressure in ulnar-humeral discrepancies, it is necessary to know the biomechanical parameters. It remains to be seen whether TSDM can reverse disease progression, prevent cartilage damage or fragmentation of the MVO at the fracture site, or reduce persistent abrasion medial section after subtotal osteotomy of the coronoid process due to friction. Also at this stage it is unknown whether TSDM can be used for successful palliative treatment last stage erosions of the medial compartment, when periarticular fibrosis or the depth of pathology can level out positive effect releasing the tendon. Conservative treatment remains the main alternative in cases where local surgical intervention is not suitable or has already been carried out, but did not lead to the disappearance of symptoms. Successful non-surgical treatment plans include regular moderate physical exercise, body weight control; prudent use of nonsteroidal anti-inflammatory drugs or prescription pain medications; application food additives or compounds that influence the course of the disease (for example, the most promising drugs are glucosamine and chondroitin sulfate, or compounds such as pentosan polysulfate). Additional therapy, including limited strength training (eg, hydrotherapy), should also be considered; physiotherapy, such as massage; transcutaneous electrical nerve stimulation; shock wave therapy, holistic, magnetic or alternative therapy, for example, acupuncture. Although scientific evidence The effectiveness of many of these methods is insufficient; a large amount of data on their use for the treatment of other animal species and low morbidity justify their use in individual cases.
Algorithm for choosing a treatment method for MVO lesions
According to our current algorithm (Fig. 4), subtotal osteotomy is indicated at the final stage of the process, when arthroscopy reveals changes such as fragmentation, large cracks, or sclerosis of the full thickness of the articular cartilage. If arthroscopy reveals early stage or mild degree lesions of the MVO, usually in the form of formation of fibrocartilage on the surface or softening of the cartilage, which is often limited to the most craniomedial part of the coronoid process, before deciding on a subtotal osteotomy, TSDM or conservative treatment other factors need to be taken into account.These factors must be weighed by answering 3 questions:
1.Is the pathology of the subchondral bone sufficient significant reason lameness or tenderness justifying subtotal osteotomy despite the absence of superficial pathology?
2. Do arthroscopic changes indicate possible rotational instability manifested by pathological changes in the area of the radial notch, which justifies TSDM in an attempt to reduce the forces acting on the joint during supination?
3. Is the observed pathology likely to progress to the final stage of MVO lesions with lameness or pain if left untreated?
When deciding on subtotal osteotomy of the coronoid process in case of questionable arthroscopy results, 2 factors are most important: severity clinical signs(lameness and tenderness on manipulation) and young age (when skeletal immaturity is considered a significant predictor of subsequent development of end-stage MVO lesions).
In addition, changes on the x-ray (including the subjective intensity of sclerosis at the trochlear notch), the ability of the owner and dog to comply with conservative treatment regimens, and the response to previous attempts at conservative treatment should be taken into account. For example, according to our algorithm, a 6-year-old dog with mild elbow lameness or tenderness and superficial localized fibrocartilage formation at the apex of the coronoid process would be treated conservatively, while a 6-month-old dog with moderate lameness associated with superficial lesion medial surface of the coronoid process of slight severity, visible during arthroscopy, and intense tissue sclerosis under the trochlear notch, visible on x-ray, a subtotal osteotomy of the coronoid process or TSDM is indicated depending on the degree of pathology of the medial coronoid process (fibrillation, cracks, fragmentation).
The sliding scale analogy is most useful when you need to consider these variables (Figure 5) in combination; in some cases there may be a slight degree of subjectivity. There is no doubt that ongoing research aimed at classifying and establishing the meaning of lesions bone marrow MVR using MRI and CT will help eliminate this subjectivity. Comparison of changes seen on x-ray or arthroscopy with the results of micro-CT and histomorphometric analysis of excised coronoid fragments will also help clarify the relationship between incongruity and morphological changes and help develop future decision-making algorithms.
LESIONS TO THE MEDIAL CONDYLE OF THE HUMERUS
OX (and resulting ROX) – good known disease medial elbow joint, which often occurs in combination with MVO lesions (30/33 elbows in one of our studies 45 ). This may reflect the possible role of incongruity in the etiology and pathogenesis of both diseases, although multiple developmental factors play a role, including genetic factors 46 , 47 ; food 48; growth rate 49 and endocrine factors 50 . Many studies describe the treatment of these two diseases together, but they do not reflect the full spectrum pathological changes, found in our dog population. In particular, we often encountered MVO lesions in combination with erosion of the cartilage of the medial condyle of the humerus varying degrees, apparently associated with MVO lesions, which further confirms the role of incongruity in etiology and pathogenesis. These erosions are visible at arthroscopy or arthrotomy as clusters of linear areas of abrasion/streaks with an axial orientation, and the pattern can vary from superficial fission of the cartilage to full-thickness sclerosis with exposure of subchondral bone. In addition, the area of the affected surface of the medial humeral condyle varies considerably, from limited areas of a few millimeters in diameter to erosion across almost the entire medial surface of the articular cartilage. These lesions are often located around or directly adjacent to the affected surface of the MVO, but remain clearly visible as appearance, and by the depth of the subchondral bone defect. The pattern of cartilage damage in the medial aspect of the coronoid process is always similar within the same surface area (mirror image), while additional macroscopic fragmentation or fissure formation, although more common, is more variable.With both surgical and conservative treatment of ROC of the medial condyle of the humerus (with or without MVO involvement), the progression of osteoarthritis is inevitable, 3 however different variants outcomes within the spectrum of the diagnosed disease, as well as detailed results in the medium and long term, are not described in most sources. In our experience, the presence of significant cartilage damage to the medial humeral condyle is associated with relatively poor clinical outcomes and, in some cases, may continue to progress to full-thickness erosion of the medial aspect of the joint, even with concurrent treatment of MVO with subtotal osteotomy. In some cases, a relatively equal distribution of load between the large contact area of the shoulder and shoulder contributes to the severity of the lesion. radius and a small contact area between the humerus and ulna in the normal elbow 51 . It seems unlikely that the growth of fibrocartilage from the subchondral bone into this area (which is stimulated by bone threfination) will provide any significant or lasting protection to the subchondral bone plate, especially given its weight bearing, constant friction, and any possible dynamic incongruity. This outcome was confirmed by the results of repeated revision of arthroscopy results in a number of cases in which only fragment removal, curettage, treatment of cartilage microcracks or trefination were performed 24 . Thus, a number of treatments have been proposed for these problematic medial humeral condyle injuries, and the algorithm for selecting a technique has become relatively complex (Fig. 6) 34,52.
ROH
When ROC is detected in the absence of MVO lesions or erosion of the corresponding medial humeral condyle, the choice of treatment options is relatively simple. The pathology of MVO can be excluded mainly based on the results of arthroscopy (lack of softening of the cartilage, fiber disintegration, cracks and fragmentation). However, in cases where these end-stage manifestations of MVO lesions have not yet developed, despite significant pathology of the subchondral tissue, especially in young dogs, the results of radiography should also be taken into account, in particular the absence of abundant or intense sclerosis in the area under the trochlear notch or coronoid process 22 ,53. Traditional methods surgical treatment (including curettage, microfractures, micropunctures) aimed at stimulating the growth of fibrocartilage is still considered justified for the treatment of small (maximum diameter<5 мм у собак средних и крупных размеров), мелких (дефект подхрящевой кости на глубину<1 мм) или абаксиальных поражений, когда прогноз, исходя из опыта, расценивается как относительно благоприятный. Опыт показывает, что при более значительных поражениях большего диаметра, с глубоким дефектом подхрящевой ткани или регенерацией с образованием волокнистого хряща такой метод недостаточен и не обеспечивает достаточной реконструкции контура сустава. Возможными причинами неблагоприятного клинического исхода считаются два аспекта: Во-первых, полагают, что по сравнению с гиалиновым хрящом, волокнистый хрящ с худшими механическими свойствами способствует снижению прочности в средне- и долговременной перспективе, что в конечном итоге приводит к склерозу, повторному обнажению подхрящевой кости и рецидиву хромоты.Second, and perhaps more importantly, accurate restoration of the weight-bearing contour with fibrocartilage is unlikely, especially when there are significant defects in the subchondral bone plate. This may promote persistent tension around the residual defect, 54 resulting in cartilage abrasion, subchondral bone swelling, and damage to the opposing articular surface. As a result, although not proven in dogs, it may be a major cause of poor outcome, particularly because the elbow joint may involve a significant portion of the limited weight-bearing surface. Reconstruction of the joint contour is the primary goal of reconstructing osteochondral defects in humans, and a number of materials (autografts, foreign grafts, absorbable and nonabsorbable fillers) have been investigated for this purpose. Of the techniques available for practical use, the use of osteochondral autograft is the best suited for dogs. In this case, a cylindrical fragment is taken from the bone of the non-contact surface of the other joint of the dog, covered with intact cartilage (usually from the area of the medial articular surface of the knee joint), which is implanted into the depression created at the site of the osteochondral defect (Fig. 7). This procedure accurately restores the contour of the joint and subchondral bone, and creates a durable surface of hyaline or hyaline-like cartilage. 45
By using polyurethane “cartilage substitute” plugs, graft removal from the donor site can be eliminated, operative time can be reduced, and the complexity associated with surface topographic mapping can be reduced.
(B) Arthroscopic image 12 weeks after surgery showing the healthy appearance of osteochondral autograft cartilage (right side of the image) used to treat an OCD lesion of the medial humeral condyle without associated MVO lesion. Photographs of the elbow joint of a Labrador retriever at the age of 3 years 8 months, who had previously undergone surgery to close the defect of the humeral condyle due to ROC with an autograft, in craniocaudal (C) and mediolateral (D) projections, without signs of progress of periarticular osteophytosis.
Such techniques are the subject of ongoing research, and mid-term (6-month) outcome measures based on clinical trial, arthroscopy, and MRI are encouraging. 55 Our clinical and arthroscopic results for 3 elbows diagnosed with MVO after autograft were excellent (Figure 7B), and follow-up of one dog for up to 3 years showed no progression of osteoarthritis (Figure 7C and D ). 45
ROH and the defeat of the MVO
ROH– the most common pathology, found in combination with MVO lesions in one joint. In this case, the treatment approach is based on the severity of the cartilage pathology, simultaneous damage to the coronoid process and the medial condyle of the humerus around or near the focus of RCD. When a MVO lesion is detected in combination with ROC of the medial condyle of the humerus, we consider subtotal osteotomy to be justified, regardless of the severity of the pathology on arthroscopy or radiography.This approach is based on an understanding of the role of incongruence or point loading in the etiology and pathogenesis of both diseases, which can interfere with healing after treatment of OCD with any chosen method. We have not explored the possible significance of TSDM in this aspect. Subsequently, these doubts were confirmed by the insufficiently good results of treatment of 10 of 24 elbow joints with concomitant ROC and MVO lesions using subtotal osteotomy and autotransplantation. 45
After 12-18 weeks, arthroscopic exploration revealed progression of the cartilage pathology of the medial humeral condyle around the graft site (and the corresponding contact area of the medial articular surface of the ulna proximal to the subtotal osteotomy site). In our opinion, this is caused by a discrepancy between the ulna and radius 39 ; Thus, in a subsequent series of joints with MVO and ROC lesions without additional erosions of the medial humeral condyle, we used a combination of autografting, subtotal osteotomy, and proximal osteotomy of the ulna. The outcome on clinical examination and arthroscopic exploration appears promising, and the inclusion of ulnar osteotomy in the treatment approach is likely responsible for this outcome. 45
Proximal osteotomy of the ulna. Although the optimal configuration, proximal-distal orientation, and need for intramedullary stabilization during ulnar osteotomy have not been established in the clinical setting, we believe a number of characteristics are important. Using an in vitro model of elbow joint incongruity, it was shown that distal osteotomy of the ulna does not restore congruency of the articular surface due to a strong interosseous ligament, while proximal osteotomy gives a better effect. 56
To prevent excessive inclination of the proximal segment of the ulna due to the pulling force of the biceps brachii muscle on the olecranon, to minimize the likelihood of delayed union after osteotomy, and to reduce excessive callus formation as a result of inevitable instability at the sites of transverse osteotomy, oblique osteotomy in the caudoproximal- craniodistal direction 2.
In vitro simulation of limb loading with oblique osteotomy without intramedullary fixation leads to varus deformity. If these effects are thought to be clinically insignificant, 57 prophylaxis with intramedullary stabilization has been suggested, 58 but is associated with some increase in complications (eg, pin breakage). 59 Therefore, we used an oblique configuration of the proximal ulnar osteotomy from caudoproximal to craniodistal (approximately 40° long axis) and proximolateral to distomedial (approximately 50° long axis). 45 The results of this method of osteotomy without an intramedullary pin to correct radius-ulna discrepancy and conditions such as olecranon nonunion (with a self-locking screw to secure the fragments) are promising, as they indicate reliable bone fusion without excessive callus formation and a positive clinical outcome . 60
Elbow dysplasia in dogs is a polygenically inherited disease that leads to a pathological structure of the joint, improper articulation of the head of the humerus and the sockets of the radial bones. Due to the incorrect structure, the joint quickly wears out, and progressive arthrosis occurs.
The elbow joint is created on one side by the ginglim-shaped head of the humerus, and on the other side by the articular cavity of the radius and the lunate notch of the ulna. The shape of the joint allows only bending along the body, but at the same time creates a high range of motion - up to 120o.
The semilunar notch fixes the head of the humerus and is a guiding block for flexion and extension. On the ulna you can see the uncinate process, which gives the glenoid cavity a crescent shape and also limits movement when extending the limb.
Please note right away that there is no diagnosis of “dysplasia”. Dysplasia is a collective name for several similar pathologies.
The term itself refers to the abnormal development of bones, organs, tissues and body parts. This is a general definition of all anatomical pathologies that form in the embryonic and postnatal period.
Elbow dysplasia includes 4 types of pathologies:
- Fragmentation of the olecranon process, that is, its separation from the ulna.
- Chipping of the coronoid process.
- Disconnection of the uncinate process
- Osteochondritis dissecans.
- Mechanical discrepancy between the bones of the joint (discongruence).
As a result, it develops arthrosis and lameness, the symptoms for all pathologies are identical, so they can only be distinguished on an x-ray.
Causes of pathology
Dysplasia is caused by irregular and uneven growth of the bones of the elbow joint. As a result, the depth or shape of the glenoid fossa changes, which is why the head of the humerus does not fit into the socket and oscillates in it. The head may fit tightly into the articular fossa, but the load is distributed unevenly. Because of this, the cartilage of the joint begins to wear out, and arthrosis develops.
The main reason is genetic abnormalities. A predisposition to the disease has been identified in some breeds of dogs, mainly in large pets with large body weight.
It has been noted that dogs up to 25 kg never suffer from dysplasia, since the development and growth of their musculoskeletal system is uniform, without sudden jumps.
Pathology of the structure begins to be observed between 4 and 5 months of age, at this time the pet’s growth reaches its peak, the first, while minor, symptoms are visible from 4 to 8 months of the dog’s life. Due to the uneven development of the bones of the elbow, its normal structure is disrupted, which leads to overload in certain places of the joint and arthrosis.
Thus, there is no direct genetic predisposition, but large height and weight in itself is a predisposing factor. The second factor in the development of dysplasia is an unbalanced diet in the period from 4 to 5 months, due to which the bones of the elbow joint grow unevenly.
It is worth noting that often an additional factor in the development of the disease is an excess of calcium, phosphorus or vitamin D in the diet, which owners, oddly enough, introduce into the menu precisely to avoid the development of dysplasia. Thus, it is not the lack of these elements that increases the risk of developing pathology, but an overall unbalanced diet.
Symptoms of dysplasia
The first sign is lameness – appears between 1-2 years. The animal cannot run; lameness may be on both front legs or only one. The muscles of the diseased limb gradually atrophy. Due to the increased load on a healthy paw, arthrosis can also develop in it. An x-ray is sufficient to make a diagnosis.
Lameness can be detected between 4-10 months, but more often owners notice symptoms at 10-12 months of a pet’s life.
Lameness should be suspected when:
- the dog refuses to follow the command “give me your paw”, although it used to do it easily;
- whines when trying to examine and feel the elbow joint;
- the pet is afraid to go down the stairs, does it sideways, or simply refuses to go down;
- The dog stopped running, although it used to play active games with pleasure.
Signs are also visible when palpating the joint:
- crepitus is heard during passive flexion and extension of the joint, and the dog becomes anxious due to pain;
- thickening of the joint and bones in it is detected;
- effusion is felt in the joint with lateral eversion;
- in severe cases, the joint even looks abnormal in appearance;
- muscles may become tight.

It should be remembered that dysplasia usually develops on both front legs at once. The disease can be asymptomatic in the presence of minor disorders, for example, with fragmentation of the internal coronoid process. Symptoms intensify after active games, long walks, and training.
Painful sensations are not caused by dysplasia, but osteoarthritis, therefore, the extent of the pathological process depends on the condition of the cartilage:
- First degree(sometimes called zero) – the presence of dysplasia in the complete absence of pathologies in the structure of cartilage.
- Second degree(sometimes called borderline) - on x-ray you can find areas of compaction - sclerosis. The animal feels well, but after increased exercise there is slight lameness.
- T third degree(in some sources the first) – individual osteophytes no larger than 2 mm in size are found. The dog limps constantly and behaves restlessly when the joint is palpated.
- Fourth degree(in some sources the second) - osteophytes ranging in size from 2 to 5 mm are visible in the picture. The dog cannot move the affected limb and experiences severe pain with passive movement.
- Fifth degree(sometimes called the third) – osteophytes larger than 5 mm are recorded. The pet is unable to move its paw; often this cannot be achieved even through passive movement during anesthesia, since large osteophytes block the movement of the bones of the joint.
Diagnosis of dysplasia
Both front paws are examined on x-rays, as dysplasia usually develops in both limbs. Typically, dysplasia is not difficult to diagnose:
- The mediolateral view is suitable for diagnosing fragmentation of the uncinate or olecranon process.
- To diagnose osteochondritis dissecans, a craniocaudal oblique projection is needed.
- To establish the incongruity of the joint bones, the craniocaudal and mediolateral projections are most suitable.
It is much more difficult to detect fragmentation of the coronoid process. For this, a craniocaudal projection is used, but even with such an image, the severed coronoid process is not always visible; it can only be detected with a high-quality image. Therefore, in the absence of other forms of dysplasia and in the presence of secondary signs (osteophytes, cartilage sclerosis), fragmentation of the coronoid process is diagnosed.
When diagnosing, it is important to assess the general condition of the joint, which is not always possible to do using x-rays, so macroscopic and microscopic examinations are performed examination of joint synovial fluid.
Norma is a straw-yellow liquid of normal viscosity, with no more than 3000 cells per microliter, of which 90% are band cells. With fragmentation of various processes, as well as with arthrosis, the number of cells increases to 10,000 per microliter, the synovial fluid becomes viscous, with impurities of fibrin, and sometimes blood.
Treatment of the disease
Effective treatment without surgery is impossible; conservative methods give results only in every third case and only with fragmentation of the coronoid process. Other types of dysplasia require surgery.
Symptomatic therapy
To slow down the development of osteoarthritis and pain relief, the following methods are used:
- The dog is prescribed a diet to reduce body weight, this reduces the load on the joint.
- Chondroprotective drugs are prescribed, but they are effective only in the second degree of osteoarthritis and partially in the third.
- Intra-articular injections of hyaluronidase are prescribed.
- Analgesics and non-steroidal anti-inflammatory drugs are used for pain relief, but their effect is twofold, as the dog will increase the load on the joint, which will accelerate degeneration.
- Physiotherapy procedures are used: electrophoresis, electrical stimulation, hydrotherapy and others.
Corticosteroids should not be prescribed due to their negative effects on the structure of cartilage.
Surgical treatment
Depending on the exact diagnosis, surgical treatment of elbow dysplasia may consist of various procedures:
- Fragmentation of the olecranon process. Initially, they try to secure it with a screw; unfortunately, this method is often ineffective; in this case, the olecranon process is simply removed.
- Fragmentation of the coronoid process. It is simply removed, this is enough for the disease to stop progressing.
- Fragmentation of the uncinate process. Usually the uncinate process is removed, since its reattachment with a screw is almost impossible.
- Osteochondritis dissecans. First, all fragments are removed from the joint cavity, abrasion is carried out if necessary, then a course of chondrostimulation is prescribed to restore cartilage tissue.
- Discongruence of joint bones. It is often not treated due to the complexity of the operation. But with some experience of the surgeon, he can perform reconstructive surgery or resort to other methods (arthroscopy, dynamic osteotomy). Their goal is to change the direction of load in the joint.

What to do and what surgery to prescribe is decided by the doctor based on an accurate diagnosis. But owners need to remember that surgical treatment is not capable of restoring articular cartilage; it only eliminates the cause of osteoarthritis. Therefore, after surgery, a course of rehabilitation therapy is necessary.
Prevention of dysplasia
Since the disease is inherited, the best method of prevention is to exclude dogs with dysplasia from breeding work. Unfortunately, this method is not effective enough, since the reason is not the presence of genes itself, but the large height and body weight of some breeds.
Treatment is most effective when dysplasia is detected early, so it is advisable to x-ray large breed dogs at 5-6 months for signs of dysplasia, regardless of symptoms.
