Prolapse (protrusion and incomplete closure) of the mitral valve is one of the most common incidental findings during cardiac ultrasound, which in most cases does not pose any threat to life and does not require any special treatment.
As a rule, mitral valve prolapse does not manifest itself with any symptoms, and therefore is discovered accidentally during echocardiography (ultrasound of the heart) for other reasons. In rare cases, people with mitral valve prolapse may experience intermittent pain in the chest, “interruptions in the heart,” rapid heartbeat and some other symptoms.
In order to determine whether there is a need for treatment of mitral valve prolapse, special examinations are performed: cardiac ultrasound (echocardiography), ECG. Holter ECG (recording of heart function during the day), etc. Using these diagnostic methods, doctors find out whether blood circulation in the cavities of the heart is impaired, and if so, how much.
In most cases, mitral valve prolapse does not cause serious violations blood circulation and therefore does not require special treatment. In such situations, mitral valve prolapse is more correctly considered a feature of the development of the heart, rather than a disease. Congenital and completely harmless mitral valve prolapse occurs in more than 20% of all healthy people.
People with mitral valve prolapse can live their entire lives without knowing they have this feature. In rare cases, when a heart examination reveals severely impaired blood circulation or an abnormal heart rhythm (arthymia), drug treatment may be recommended.
Surgical treatment of mitral valve prolapse (heart surgery) is required in extremely rare cases, when gross violations heart valve function.
What is a heart valve?
The heart is a kind of pump that causes blood to circulate throughout the body. This becomes possible by maintaining pressure in the cavities (chambers) of the heart. The human heart has 4 chambers: 2 ventricles and 2 atria. Valves are special valves located between the chambers of the heart, regulating the pressure in the chambers of the heart and maintaining the movement of blood in the desired direction.
There are 4 valves in the heart:
- The mitral valve is located between the left atrium and the left ventricle. This valve consists of two valves: anterior and posterior. Prolapse of the anterior mitral valve leaflet is more common than prolapse of the posterior leaflet. Attached to each valve leaflet are thin threads called chordae. These threads, in turn, are attached to small muscles (papillary, papillary muscles). For normal functioning of the valve, the joint work of the leaflets, chords and papillary muscles is necessary. During the contraction of the heart, the pressure in it increases greatly. Under the influence of this pressure, the mitral valve opens the leaflets, which are held in place by the chordae and papillary muscles.
- The tricuspid (three-leaf) valve consists of 3 leaflets and is located between the right atrium and the right ventricle of the heart.
- The aortic valve is located between the left ventricle and the aorta and prevents blood from returning back into the ventricle.
- Valve pulmonary artery located between the pulmonary artery and the right ventricle and also prevents blood from returning to the right ventricle.
How do heart valves work normally?
The left ventricle has 2 openings: one communicates with the left atrium (the mitral valve is located here), the second communicates with the aorta (the aortic valve is located here). Blood moves through the heart in the following direction: from the atrium through the open mitral valve to the ventricle and then from the ventricle through the open aortic valve to the aorta. To ensure that during contraction of the left ventricle the blood does not return back to the atrium, but moves into the aorta, the mitral valve closes tightly. As the ventricle relaxes, the aortic valve closes and blood cannot return back to the heart.
The tricuspid (three-leaf) valve and the pulmonary valve operate on the same principle. Thus, thanks to normal functioning The heart valves move blood through the chambers of the heart and maintain blood circulation throughout the body.
How do heart valves work during prolapse?
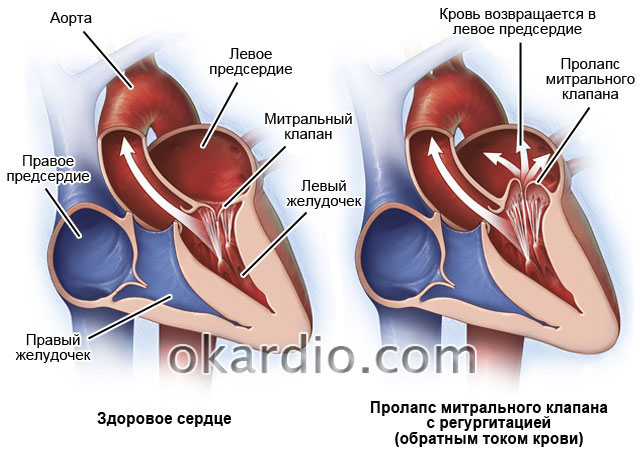
Prolapse is a bulging (bulging) of the valve leaflets during its closure, which makes the closure of the leaflets loose and allows some blood to return back, from the ventricle to the atrium or from large vessels to the ventricles.
Thus, with mitral valve prolapse, during contraction of the left ventricle, blood flows not only into the aorta, but also returns to the left atrium. This return of blood is called regurgitation. Depending on the volume of blood returned back to the atrium, several degrees of regurgitation are distinguished. Typically, mitral valve prolapse leads to very minor regurgitation, which cannot seriously impair the functioning of the heart and is considered normal.
Why does mitral valve prolapse occur?
There are 2 main causes of mitral valve prolapse: congenital and harmless prolapse and prolapse that occurs due to other diseases and injuries of the chest.
Congenital and harmless prolapse
In the vast majority of cases, the development of mitral valve prolapse is associated with congenital disorder structure and weakening of the connective tissue that makes up the heart valves.
This disorder is usually inherited and is already present at the birth of the child. Due to the weakness of the connective tissue, the valve leaflets are more easily stretched, and the chords that hold them lengthen. For this reason, when the valve closes under the influence of blood pressure, the valves protrude and do not close tightly.
Congenital mitral valve prolapse in the vast majority of cases proceeds favorably, does not cause any symptoms and does not require special treatment. In this case, prolapse is more a feature of the body than a disease.
Various heart diseases that disrupt the normal structure of the valves
Rarely, mitral valve prolapse can occur against the background of various heart diseases (acquired prolapse) that disrupt the structure of the valves, chords or papillary muscles:
- Mitral valve prolapse due to rheumatism (rheumatic heart disease, or rheumatic carditis) is more common in children and is caused by inflammation of the connective tissue that makes up the valve leaflets and chordae. As a rule, shortly before the detection of mitral valve prolapse, the child experiences a sore throat or scarlet fever, followed approximately 2 weeks later by an attack of rheumatism (inflammation large joints, pain, stiffness in joints, etc.).
- Mitral valve prolapse in the background coronary disease heart disease or myocardial infarction develops in older people, as a result of poor blood supply to the papillary muscles or rupture of the chordae regulating the functioning of the valve. Prolapse in this case is detected during examination for severe pain in the heart, shortness of breath and weakness.
- Mitral valve prolapse after chest trauma is caused by rupture of the chordae and, as a rule, has an unfavorable course if left untreated.
Congenital and acquired mitral valve prolapse have fundamentally different signs, symptoms, course and require different approaches to treatment, and therefore we will consider them separately.
Congenital mitral valve prolapse
As mentioned above, congenital mitral valve prolapse is present in a child from birth. In this case, mitral valve prolapse is often combined with a dysfunction nervous system, called vegetative-vascular dystonia (VSD). It is VSD, and not prolapse, that causes the appearance of some symptoms that are often “attributed” to prolapse:
- Periodic pain behind the sternum and in the heart area. Chest pain with mitral valve prolapse is functional character(that is, they are not a sign of a disorder of the heart) and are caused by a disorder of the nervous system. Often, pain in the heart area occurs after stress, emotional tension, and sometimes at rest. The pain can be tingling or aching and lasts from a few seconds to tens of minutes, several hours or days. Important! pain in the heart with mitral valve prolapse does not increase with physical activity, and is not combined with shortness of breath, dizziness or fainting (loss of consciousness). If you have pain in the heart area accompanied by such symptoms, consult a doctor, as they may indicate a disturbance in the functioning of the heart without a background of serious illness.
- Attacks of rapid heartbeat, or a feeling of “failure” or “fading” of the heart. These sensations are also explained increased activity nervous system and do not indicate a violation of the heart. Important: attacks of rapid heartbeat during mitral valve prolapse occur suddenly and pass just as suddenly, and are not combined with dizziness or loss of consciousness.
- Fainting with mitral valve prolapse is rare and is often associated with emotions (for example, fear) or occurs in stuffy rooms. Such fainting passes quickly after access to fresh air or a pat on the face.
- Other symptoms and signs of VSD, such as low-grade fever, headaches. abdominal pain (irritable bowel syndrome), etc. Read more about VSD in the article All about VSD and its treatment.
Often people with mitral valve prolapse have a similar body type: long, thin arms and legs, high growth, increased mobility in joints, elongated face, etc.
Since connective tissue is present in the skin, muscles and tendons, its defect can lead to strabismus, decreased visual acuity and some other features that are often combined with mitral valve prolapse.
Diagnosis of mitral valve prolapse
As a rule, congenital mitral valve prolapse is detected accidentally, at any age, during ultrasound of the heart (echocardiography). Ultrasound of the heart is the most effective method diagnosis of prolapse, as it allows you to determine the degree of prolapse and the volume of regurgitation (backflow of blood from the left ventricle into the atrium).

Degrees of mitral valve prolapse:
Grade 1 prolapse indicates slight protrusion of the mitral valve leaflets (up to 5 mm)
Grade 2 indicates bulging of the valves up to 9mm.
Stage 3 - valve flaps bulge by 10 mm or more.
The division of mitral valve prolapse into grades does not reflect the magnitude of regurgitation and is therefore not currently used to determine prognosis and indications for treatment. Much more attention is paid to the degree of mitral valve regurgitation (the amount of blood flowing back into the atrium due to incomplete closure of the valve leaflets), which is determined separately during an ultrasound.
If necessary, the doctor may prescribe additional methods for diagnosing heart function: ECG and Holter ECG. ECG allows you to see possible changes in the work of the heart, caused by mitral valve prolapse. Holter ECG is a recording of data on the work of the heart for 24 hours. As a rule, with congenital mitral valve prolapse, the functioning of the heart is not impaired and additional diagnostic methods do not reveal significant abnormalities.
How do you know how serious mitral valve prolapse is?
Only a specialist who knows your medical history and has a complete understanding of all the examinations that were performed on you can assess the degree of heart dysfunction and identify indications for treatment.
If you have mitral valve prolapse, which was discovered incidentally during an examination for another reason, you do not have such severe symptoms illness (severe pain in the heart during physical activity, dizziness, shortness of breath, significant decrease in performance) and after the examinations the cardiologist does not prescribe any treatment, then mitral valve prolapse should be considered a normal variant that cannot cause serious harm to health and does not require treatment .
Mitral valve prolapse in children
Mitral valve prolapse is often found in childhood accidentally, during an ultrasound of the heart. In addition to mitral valve prolapse, a child may experience changes such as: additional chord, accessory papillary muscles, prolapse of other heart valves (tricuspid, aortic or pulmonary valve), open oval window etc. All these changes are included in the Minor Anomalies of the Heart Syndrome (MARS).
The discovery of mitral valve prolapse and/or MARS in a child should not put parents into a state of panic, since these changes do not affect the functioning of the heart and almost always have a favorable course.
In extremely rare cases, MARS in a child may be complicated by a disturbance in the rhythm of the heart (arrhythmia) or the development infectious inflammation heart valves (infective endocarditis), and therefore children with this feature are recommended to have a preventive examination by a cardiologist 1 or 2 times a year.
Mitral valve prolapse in pregnant women
Mitral valve prolapse does not affect the course of pregnancy and childbirth and almost never leads to the development of serious complications.
However, if you have mitral valve prolapse and are planning a pregnancy or are already pregnant, be sure to tell your gynecologist. If necessary, you will be recommended for additional consultation with a cardiologist.
Treatment of congenital mitral valve prolapse
Congenital mitral valve prolapse does not require special treatment. People with mitral valve prolapse can live a full life, play sports and not limit themselves in physical activity.
Children with mitral valve prolapse are also recommended to exercise, play outdoor games, and swim (unless your doctor has discussed this separately). The decision on admission to professional sports is made individually with the attending physician.
If you have complaints of frequent palpitations, periodic heart pain, headaches, anxiety, insomnia, etc. you may be recommended one of the herbal-based sedatives (for example, valerian, Novo-passit, mint tea, etc.) These drugs normalize the functioning of the nervous system, reducing or eliminating the main symptoms of mitral valve prolapse and vegetative-vascular dystonia (VSD) .
Medicines containing magnesium (Magnesium B6, Magnerot, etc.) can also be prescribed for mitral valve prolapse and have approximately the same effect as sedatives.
In some cases, when prolapse is accompanied by a significant disruption of the heart, which is manifested by weakness, shortness of breath, seizures severe pain in the heart area during physical activity and is confirmed by cardiac ultrasound by significant regurgitation, a cardiologist may recommend more serious drug treatment, including medications that normalize the rhythm of the heart and some others. Let us repeat that the need for such treatment is determined strictly individually by the attending cardiologist.
Mitral valve prolapse due to heart disease
As mentioned above, mitral valve prolapse can develop against the background of a number of heart diseases, or less commonly as a result of chest injuries.
If mitral valve prolapse was detected on a cardiac ultrasound after a recent sore throat, scarlet fever or an attack of acute rheumatic fever (pain, swelling, redness of large joints, etc.), then there is a high probability that this is one of the complications rheumatic lesions heart (rheumatic carditis).
The main symptoms of mitral valve prolapse in this case are:
- Increased fatigue, weakness, passivity of the child, refusal of active games.
- The appearance of shortness of breath after normal physical activity.
- Rapid heartbeat, dizziness.
Treatment of mitral valve prolapse in this case is carried out in a hospital setting. Since the cause of inflammation of the heart valves is a bacterium (streptococcus), treatment with antibiotics from the penicillin group (penicillin, bicillin, etc.) or other groups is recommended. If a cardiac ultrasound reveals severe regurgitation or cardiac arrhythmia, other medications are also used. In this case, treatment is prescribed by the attending rheumatologist.
If, as a result of rheumatic inflammation of the heart (rheumatic carditis), severe mitral valve insufficiency develops, which cannot be treated drug treatment, a surgical operation is performed on the heart with replacement (prosthetics) of the valve.
If mitral valve prolapse is detected in an elderly person with coronary heart disease (CHD, or angina), then probable cause its development is poor blood supply to the papillary muscles, caused by the underlying disease. The main symptoms in this case are:
- Attacks of severe pain in the heart area, which disappear after taking nitroglycerin.
- Shortness of breath with minor physical exertion.
- “Interruptions” in the work of the heart, a feeling of cardiac arrest, etc.
In this case, treatment of coronary heart disease (angina) is necessary, aimed at normalizing the blood supply to the heart, reducing arterial hypertension (high blood pressure) etc. see Treatment of coronary heart disease.
Mitral valve prolapse found after recent chest trauma may be caused by rupture of the chordae or papillary muscles. The main symptoms of prolapse in this case include:
- “Interruptions” in the work of the heart, rapid heartbeat.
- Weakness, shortness of breath after minor physical activity or at rest.
- A cough with pink, frothy sputum may appear. If this symptom occurs, you should call as soon as possible ambulance, since delay in treatment can lead to death.
Treatment of mitral valve prolapse as a result of chordal rupture is carried out in the hospital, under the close supervision of specialists. After normalization of the condition with the help of medications, as a rule, heart surgery is recommended, during which the patient is restored. normal operation valve
Possible complications of mitral valve prolapse
Complications of mild congenital mitral valve prolapse are extremely rare.
More often, complications arise against the background of severe congenital prolapse and prolapse that occurs against the background of other heart diseases (for example, rheumatism) and chest injuries:
- Mitral valve insufficiency is common complication rheumatic inflammation of the heart (rheumatism), meaning incomplete closure of the valve leaflets and large quantity blood back into the atrium. The main signs of mitral regurgitation are: weakness, shortness of breath, increased fatigue, cough, etc. Ultrasound of the heart allows you to clarify the presence of mitral regurgitation. In order to eliminate mitral valve insufficiency, heart surgery with mitral valve replacement is recommended.
- Arrhythmia is a disturbance in the rhythm of the heart, which leads to dizziness, weakness, a feeling of “interruptions” in the work of the heart and even short-term fainting. Antiarrhythmic drugs (Amiodarone, Atenolol, etc.) are used in the treatment of arrhythmia.
- Infective endocarditis is a very serious complication that is characterized by inflammation of the heart valve. The main signs of this disease are: increased body temperature, severe general weakness, aching pain in the joints. possible reduction blood pressure, rapid heartbeat, jaundice of the skin, etc. More often, infective endocarditis develops after dental procedures(tooth extraction, filling, etc.), or other surgical interventions. Treatment infective endocarditis carried out in a hospital, under the strict supervision of doctors.
- Other complications of mitral valve prolapse are much less common and a preventive visit to a cardiologist with necessary examinations(for example, ultrasound of the heart) can reduce the risk of their occurrence to a minimum.
Mitral valve prolapse (MVP) - this diagnosis can often be seen in the results of cardiac ultrasound. However, you should not immediately worry: this type of valve disease is often diagnosed in completely healthy people and requires only periodic monitoring by a cardiologist.
Therapeutic tactics directly depend not only on the severity of valve prolapse (sagging), but also on the degree of regurgitation (the amount of reverse blood flow).
Mitral valve prolapse - what is it?
The mitral (bicuspid) valve separates the chambers of the left side of the heart: the atrium and the ventricle. Mitral valve prolapse is the bowing of the valve leaflets during contraction (systole) of the left ventricle.
The pathology is caused by a violation of the structure of the valve (its fibrous layer, less often the chordae tendineae) due to connective tissue dysplasia. In this case, the valve flaps not only bend, but may also not close tightly.
When the left ventricle contracts, blood rushes back into the atrium through the remaining lumen of the valve. This process is called regurgitation.
MVP is most often diagnosed in young people 20-35 years old. It is extremely rare that deviations in the structure and function of the mitral valve are found in young children. Among adults, the frequency of pathology ranges from 10-25%, and in the elderly - 50%.
Main reasons formation of a valve defect:
- Hereditary connective tissue dysplasia (Marfan and Ehlers-Danlos syndromes) - primary valve prolapse develops;
- Incorrect osteogenesis, leading to deformation of the chest;
- Rheumatic heart damage, inflammatory processes in its membranes, heart attack, chronic ischemia heart, atherosclerosis/calcification of the valve ring - secondary prolapse is formed.
According to the severity of the deflection Mitral prolapse is distinguished:
- 1st degree - the height of the dome-shaped deflection of the valves does not exceed 0.6 cm (the norm is 1-2 mm);
- 2 degrees - bulging up to 0.9 cm;
- 3 degrees - the dome of the sash is more than 0.9 cm high.
Symptoms of prolapse by degree of regurgitation
The classification of MVP according to the severity of deflection of the valve leaflets is quite arbitrary. The most important factor influencing general state person and therapeutic tactics, is the degree of regurgitation (grade 1 - 3), which causes symptomatic picture mitral insufficiency.
Mitral valve prolapse grade 0

Even with a fairly pronounced deflection, the valves close tightly, and the full volume of blood from the left ventricle enters the aorta (there is no reverse blood flow into the left atrium).
At the same time, grade 0 regurgitation does not give any painful symptoms: the person feels completely healthy and has no complaints about the functioning of the heart.

pain on exertion
Mitral valve prolapse and grade 1 regurgitation are diagnosed when the volume of blood returned to the atrium is minimal. The patient does not present any complaints indicating circulatory disorders.
Some patients report pain in the right hypochondrium while running. This is due to insufficient right ventricular functionality leading to an increase in the volume of blood flow in the heart. The deviation is recorded during the examination:
- Auscultation - listening to a murmur at the apex of the heart and a specific click caused by a sharp tension of the relaxed chords during ventricular systole. The clicks are more audible in an upright position and may disappear completely when lying down. Sometimes (not necessarily!) a “meowing” (squeaking) sound is heard, which occurs when the chordae or the valve leaf itself vibrate.
- Echocardiography (ultrasound of the heart) - a small gap between the closed valve leaflets and a fixed volume of blood returning to the atrium.
Mitral valve prolapse 2nd degree - mitral insufficiency
With bicuspid valve prolapse and 2nd degree regurgitation, ultrasound (cardiac Doppler) shows more than pronounced signs mitral insufficiency. The blood stream, returning through the incompletely closed valve, reaches the middle of the atrium chamber.
More than 25% of the blood returns to the atrium from the ventricle. In this case, symptoms characteristic of stagnation in the pulmonary circulation are observed:
- Heart pain - mild or moderate, without close connection with physical activity or an emotional reaction to stress (may occur spontaneously). Taking Nitroglycerin does not have much effect in eliminating such pain.
- The headache is intense, often bilateral (only sometimes imitates a migraine). Headache often occurs against the background of a sudden change in weather, after emotional stress.
- Shortness of breath - often caused by hyperventilation syndrome (deep or frequent breaths provoked by a feeling of lack of air). Shortness of breath can occur even after minimal physical exertion.
- Autonomic dysfunction - manifested by a lump in the throat, excessive sweating, rapid fatigue and morning weakness, an unreasonable rise in temperature to 37.0-37.5ºC, nausea and dizziness. At the same time, vegetative crises are repeated at least once a week, are not associated with situations threatening the patient, and the emotional side this state somewhat muted. Fainting can also occur extremely rarely. Autonomic disorders provoke the development depressive states and emotional instability (sadness and gloominess in the morning, anxiety and irritability in the evening). Often, patients complain of specific bodily sensations, which are sometimes perceived as a symptom of another physical disease.
- Interruptions in the work of the heart - periodically the patient notices tremors or cardiac arrest. At the same time, extrasystoles (extraordinary heart beats) and tachycardia (increased heart rate) are not recorded constantly, but occur during emotional experience, physical activity, or even after drinking coffee.
Mitral valve prolapse grade 3
Insufficiency in the pulmonary circulation leads to increased load on the right half of the heart. Existing symptoms gradually worsen and severe symptoms systemic insufficiency: edema, increased blood pressure, bluish skin, insurmountable weakness, atrial fibrillation and enlarged liver. Such patients usually receive 1 group of disability.
Mitral valve prolapse is life-threatening precisely in grade 3 regurgitation: the development of paroxysmal tachycardia, pulmonary edema, endocarditis and other severe complications, including sudden death, is possible.
Patients with bicuspid valve prolapse are more likely to get sick than others colds, they are often diagnosed with chronic tonsillitis.
- Dysplastic changes indicate congenital dysplastic pathology of connective tissue in childhood hip joints, flat feet, abdominal hernias.
Mitral valve prolapse during pregnancy
Minor prolapse of the bicuspid valve and minor mitral insufficiency are not a contraindication to pregnancy; childbearing in this case is normal.
In this case, there may even be a temporary decrease in the deflection of the valve leaflets due to a physiological increase in the size of the left ventricle. However, the systolic murmur and clicks return 1 month after delivery.
Severe regurgitation and mitral valve prolapse are more dangerous during pregnancy: the risk of developing attacks of paroxysmal tachycardia is significantly increased. During childbirth, rupture of the valve chords is not excluded.
Women with MVP often experience premature rupture of amniotic fluid and weak labor contractions. The baby is susceptible to intrauterine asphyxia and is often born with low weight (hypotrophy).
 Therapeutic tactics are chosen in strict accordance with the degree of bicuspid valve prolapse, the presence/absence of signs of mitral regurgitation and complications that arise.
Therapeutic tactics are chosen in strict accordance with the degree of bicuspid valve prolapse, the presence/absence of signs of mitral regurgitation and complications that arise.
1st degree of mitral valve prolapse: health-improving measures
With a slight change in the structure of the leaflets (mitral valve prolapse with regurgitation of the 1st degree), the absence constant arrhythmia and other painful symptoms do not require treatment. A person is recommended to be monitored by a cardiologist once a year and correct the following lifestyle habits:
- Quitting smoking and alcohol, coffee and strong tea;
- Balanced diet;
- Physical activity commensurate with the body’s capabilities;
- Cultivating stress resistance;
- Rational work-rest schedule.
Treatment of MVP and 2nd degree regurgitation
The appearance of painful symptoms of mitral valve prolapse indicates the need for drug therapy. The treatment regimen includes:
- Elimination of heart pain - it is advisable to use sedatives (valerian, sage, hawthorn, St. John's wort, motherwort);
- Therapy vegetative-vascular dystonia- antidepressants (Amitriptyline, Azafen), neuroleptics (Sonopax, Triftazin), tranquilizers (Elenium, Seduxen, Grandaxin);
- Improving metabolism in the myocardium - Riboxin, Kartinin, coenzyme Q-10, Panangin, vitamins and magnesium preparations (especially effective for mitral prolapse!);
- Recovery heart rate- Obzidan and other adrenergic blockers;
- Prevention of infective endocarditis - broad-spectrum antibiotics for each surgical intervention (tooth extraction, tonsillectomy).
Elimination of severe regurgitation due to bicuspid valve prolapse
To eliminate disease progression and prevent severe consequences for mitral insufficiency, cardiac glycosides, diuretics, ACE inhibitors(non-hypotensive dosage of Captopril - about 0.5 mg/kg body weight per day - has a cardioprotective effect). Simultaneously with drug therapy, surgical plastic surgery bicuspid valve.
Depending on the structural changes Cardiac surgeons perform shortening of valve chords, suturing of leaflets and ablation of foci of pathological impulses (elimination of arrhythmia). In severe cases, the valve is completely replaced.
Possibilities modern medicine allow many heart surgeries to be performed using endovascular (transcatheter) or endoscopic access. TO open surgery cardiac surgeons resort only in extreme cases, for example, with combined defects.
Forecast
In the absence of mitral regurgitation, the outcome of the disease is usually favorable. It is worth noting that a slight deflection of the valve leaflets in thin people and teenage children can disappear on their own if they adhere to a rest regime, appropriate physical activity and good nutrition.
Patient's health in severe cases mitral prolapse and the rapid progression of the disease directly depends on the timeliness and adequacy of medical care.
Mitral valve prolapse is a minor malformation of the valvular apparatus of the heart and in most cases is not dangerous. The severity of the disorders is judged by the results of an ultrasound examination, which shows not only the degree of valve prolapse but also the level of regurgitation (return) of blood in the atrium. Patients with mild mitral valve prolapse can live a normal life, but it is necessary to periodically undergo follow-up examinations to monitor the dynamics of the disease.
- 1. Primary MVP.
- 2. Secondary PMC.
- 1. Stage 1 MVP - the bicuspid valve leaflets prolapse no more than 6 mm. Regurgitation is minor and does not lead to severe circulatory disorders. Pathology of this degree in most cases does not manifest itself clinically and has a neutral course. Special treatment this condition does not require, but periodic examinations of the patient and ultrasound examinations are necessary. Sports and physical exercise such patients are not contraindicated, but strength exercises and weightlifting are prohibited.
- 2. Grade 2 MVP - prolapse within 6-9 mm. Available clinical manifestations diseases, such patients are prescribed symptomatic treatment. Physical education and sports are allowed only in agreement with a cardiologist, as the load must be selected correctly.
- 3. Grade 3 MVP - leaflet prolapse greater than 9 mm. In this case, severe disturbances in the structure of the heart occur. The cavity of the left atrium chamber begins to expand, and the walls of the ventricles hypertrophy. Blood is released into the aorta in insufficient volume, and severe circulatory disorders develop. Prolapse leads to heart rhythm disturbances and mitral insufficiency. In this form of the disease, surgical interventions are performed that are aimed at prosthetics or suturing of the valves. Patients with the third degree of MVP are prescribed a complex physical therapy which is carried out under the supervision of doctors.
- 1. The first stage is characterized by regurgitation at the level of the valve leaflets.
- 2. The second is characterized by the formation of a regurgitation wave that reaches the middle of the left atrium chamber.
- 3. The third stage is characterized by the appearance of a wave of blood return, reaching the opposite end of the left atrium.
- Early prolapse.
- Later.
- Holosystolic.
- PMC of both valves.
- PMC of the rear sash.
- PMC of the front leaf.
- “silent” form - pathological heart murmurs are not heard;
- auscultatory form - pathological sounds of regurgitation are heard.
- lengthening or shortening of the cardiac chords;
- improper attachment of the chords to the valve flaps;
- presence of additional chords;
- Acute respiratory viral infections during pregnancy.
- The presence of occupational hazards in a woman.
- Preeclampsia.
- Influence environmental factors on the mother during pregnancy.
- Excessive stress on the body of a pregnant woman.
- Morphan's syndrome.
- Arachnodactyly.
- Elastic pseudoxanthoma.
- Osteogenesis imperfecta.
- Ehlers-Danlos syndrome.
- Cardiac ischemia.
- Rheumatism.
- Myocarditis.
- Hyperthyroidism.
- Chest injuries.
- Hypertrophic cardiomyopathy.
- Systemic lupus erythematosus.
- Myocardial dystrophy.
- Myocarditis.
- inguinal and umbilical hernias;
- joint hypermobility;
- scoliosis;
- chest deformation;
- myopia;
- flat feet;
- strabismus;
- varicocele;
- nephroptosis;
- hip dysplasia.
- Feeling of heartbeat.
- Increased heart rate.
- Heart pain of various types.
- Collapses - a sharp drop in blood pressure as a result of disorders of the autonomic nervous system is accompanied by darkening of the eyes with the possibility of loss of consciousness.
- Dizziness.
- Nausea.
- Feeling short of breath, migraine-like headaches.
- Vegetative crises.
- Various rhythm disturbances.
- Tendency to depression.
- Synestopathies are unpleasant painful sensations in the body for which there is no explanation.
- Unreasonable appearance of asthenic syndrome (weakness, fatigue, decreased attention, memory).
- rhythm disturbances;
- tachycardia or bradycardia;
- extrasystole;
- Wolff-Parkinson-White syndrome;
- atrial fibrillation, etc.;
- Sleep should be at least 8 hours.
- It is necessary to carry out a complex of dosed physical activity.
- We need to normalize our daily routine.
- Follow the rules rational nutrition- include more vegetables and fruits in your food.
Show all
What is mitral valve prolapse?
Mitral valve prolapse
To understand pathology, it is necessary to address issues of anatomy. The mitral valve or bicuspid valve is located between the left atrium and the left ventricle. It consists of two wings, front and back. Attached to each leaflet are chordae, which arise from the papillary muscles of the ventricle and attach to the valve. These formations hold the valves and prevent them from bending into the atria during contraction of the ventricles.
During atrial systole, the mitral valve opens towards the ventricle and allows blood into it. After this, it closes and ventricular systole begins, during which blood is expelled into the arteries of the systemic circulation through the aortic valve. The job of the mitral valve is to create an obstacle to the reverse flow of blood from the ventricles, during their contraction, into the atria.
Mitral valve prolapse (MVP) is a condition in which sagging or protrusion of the posterior and/or anterior valve leaflets occurs. As a result, their closure is incomplete, and a hole remains through which blood

Anatomy of the mitral valve
is thrown (registers) back into the atrium. The severity of the condition directly depends on the degree of regurgitation.
The diagnosis of mitral valve prolapse is made only on the basis of Doppler ultrasound. Interpretation of ultrasound data should be carried out by a cardiologist together with a specialist functional diagnostics.

Classification
MVP is classified depending on the severity of prolapse, degree of regurgitation and etiology.
According to etiology there are:
Depending on the severity of valve prolapse there are:

Stages of MVP
Since the degree of regurgitation does not always depend on the severity of prolapse, three stages of mitral valve prolapse are distinguished. They are determined depending on the severity of blood return to the left atrium. The level of regurgitation is determined according to Doppler ultrasound data:
Depending on the relationship to ventricular systole, the following are distinguished:
Depending on the location there are:
Depending on the presence of auscultatory clinical signs, it is customary to distinguish:

Causes of MVP
Mitral valve prolapse is not an independent disease. It is a syndrome that occurs in numerous diseases. Depending on the etiology, secondary MVP is distinguished - it occurs as a result of other pathologies, and primary - it is also congenital or idiopathic.
Quite often, idiopathic MVP is detected in children and adolescents. It appears due to congenital connective tissue dysplasia. As a result of this disease, other disorders in the structure of the valve apparatus may develop, for example:
As a result of structural changes in the connective tissue, degenerative processes occur in the valve leaflets, and they become more pliable. Because of this, the valve cannot withstand the pressure created by the left ventricle and bends towards the left atrium. Connective tissue dysplasia can occur for various reasons that affect the child in the womb, among them the following:
In approximately 20% of cases, congenital MVP is transmitted through the maternal line. In addition, mitral valve prolapse occurs in other hereditary diseases, such as:
Secondary MVP (or acquired) can occur as a result of certain diseases. The most common causes of this pathological condition are:
Prolapse in this case occurs due to damage to the valve leaflets, papillary muscles, chordae or disturbances in the function and structure of the myocardium. Also, an important role in the mechanism of development of MVP is played by disturbances in the functioning of the autonomic nervous system, deficiency of micro- and macroelements (especially Magnesium) and metabolic pathology.
Another cause of secondary prolapse is stenosis aortic valve. As a result of this acquired defect, the opening of the aortic valve narrows, and blood cannot fully pass through it. This creates excess pressure in the left ventricle, which in turn presses on the bicuspid valve. If there is a fact of prolonged existence of excess pressure, then the mitral valve leaflets begin to bend towards the left atrium, and prolapse occurs.

Symptoms
The appearance of mitral valve prolapse with minimal changes may be absent and the pathology is detected by chance during an ultrasound examination of the heart.
Symptoms directly depend on the degree of regurgitation and the severity of connective tissue dysplasia. In children with congenital MVP, the following are quite common:
These diseases indicate the presence of disturbances in the structure of the connective tissue and very often along with them they reveal malformations of the valvular apparatus of the heart, including prolapse.
Patients with dysplasia more often than healthy people suffer from sore throats and acute respiratory viral infections.
Nonspecific symptoms of MVP are:
With severe regurgitation, patients develop shortness of breath and fast fatiguability, performance is significantly reduced and physical activity.MVP is also characterized by the occurrence of psychosensory disorders such as:
The symptoms of secondary MVP are similar to those described above, but they are accompanied by clinical manifestations of the underlying disease (rheumatism, myocarditis, coronary heart disease, etc.). Severe types of mitral valve prolapse are dangerous due to their complications such as the development of arrhythmia, thromboembolism or infective endocarditis.
In pregnant women and children
Mitral valve prolapse is much more common in children than in adults. Quite often it is registered in adolescence, And most of falls on girls. The main complaints in children are heaviness in the heart, lack of air and chest pain.
In childhood, MVP often develops due to insufficient magnesium in the body. This trace element is necessary for the production of collagen by connective tissue cells. Collagen is a substance that is responsible for the elasticity of connective tissue, and it, in turn, is the main component of the valve leaflet.
During pregnancy, grade 1-2 mitral valve prolapse syndrome in most cases does not in any way disrupt the course of the gestational period. During this period, MVP may even decrease, because at this time the woman’s cardiac output and vascular resistance decreases.
But in some cases, patients may be bothered by disturbances in the functioning of the heart, a feeling of palpitations, a feeling of lack of air, and tachycardia.
Very often severe prolapse is accompanied by gestosis. In this case, it is dangerous because the fetus’s growth slows down and oxygen deficiency occurs. Sometimes women experience premature birth or weakness develops labor activity. In such a situation, they carry out C-section.
Diagnostics
The basis for diagnosing MVP is ultrasound with Dopplerography. It allows you to identify the degree of prolapse and the severity of regurgitation. Also, using this method, stages of the disease that do not have clinical manifestations are identified.
Heart murmurs can be heard using phonocardiography or auscultation. In the case of the “silent” form of the disease, pathological noises are not heard in this way, but can be recorded on phonocardiography.
Using X-rays, you can detect changes in the size of the heart - enlargement or reduction of cavities, changes in configuration, etc.
Electrocardiography performed throughout the day (Holter heart monitoring) may show the following abnormalities:
In cases of severe regurgitation and signs of heart failure, bicycle ergometry is performed. It shows how reduced a person’s performance is and allows you to determine the degree of insufficiency.
Treatment
Treatment of MVP is carried out taking into account the severity of hemodynamic disorders and clinical manifestations. Conservative therapy is to eliminate vegetative disorders of central origin, prevent the occurrence dystrophic changes myocardium and prevention of possible complications.
Patients with severe clinical manifestations of the disease are prescribed drugs from the group of adaptogens (Eleutherococcus, Ginseng, Schisandra), sedatives plant origin(Novo-passit, Persen Fitosed) and drugs that improve the trophic function of the myocardium (Carnitine, Coenzyme, vitamins, Inosine, magnesium and potassium aspartate).
If there are symptoms of heart failure, beta blockers (Bisoprolol, Atenolol) and drugs with antiplatelet properties (Warfarin, Acetylsalicylic acid in low dosages). These remedies are taken daily for several months or years.
Patients need to normalize their lifestyle:
In case of severe hemodynamic disturbances, surgical operations are performed, which include suturing or replacement of the mitral valve.
A cardiologist should prescribe complex treatment. Also, patients with MVP need to undergo periodic examinations and monitor the course of the disease.
Traditional methods
Folk remedies can only provide maintenance therapy. It is impossible to treat prolapse on your own.
As traditional methods You can use herbal remedies that have restorative and sedative properties. For this purpose, valerian, motherwort, hawthorn fruits, and aloe are used.
These remedies eliminate disturbances in the functioning of the autonomic nervous system and strengthen the functioning of immune system.
Forecast
People with grade 1-2 mitral valve prolapse have a favorable prognosis, but supportive treatment and periodic examinations are necessary. Such patients can play sports, but strength exercises are contraindicated.
In patients with third-degree prolapse, the prognosis is less favorable, as the configuration of the heart begins to change and severe hemodynamic disturbances develop. After surgery, the likelihood full recovery quite high. Light physical activity will be sufficient for this category of patients, but it can only be performed after consultation with the attending physician.
Patients with minor changes in hemodynamics are recruited into the army. But in case of severe clinical symptoms and circulatory disorders, the service will be contraindicated.
Prolapse of the mitral valve, and in particular its anterior leaflet, occurs due to changes in the very structure of this component of the heart. Most often, such an anomaly affects the child at the stage of gestation.
Sometimes pathological process begins to develop in an adult. Lack of proper treatment leads to rapid progression of the disease and death of the patient.
Therefore, it is extremely important to know about the signs of the disease, diagnostic methods and therapy.
General idea of pathology
Mitral regurgitation (MVR) is a disease that is usually characterized by the development of an abnormal process in the connective tissue. As a result of these harmful changes, the valve weakens and loses tone.
Then, with each successive contraction of the heart ventricle, it begins to bend into the atrium cavity and does not close completely. Therefore, a small amount of blood still returns. An indicator such as ejection fraction is significantly reduced.
 An experienced cardiologist must determine how far the distance between the leaflets has deviated from the norm. Based on this observation, various degrees of mitral disease are distinguished. By the way, deflection of the front flap is much more common than deflection of the rear flap.
An experienced cardiologist must determine how far the distance between the leaflets has deviated from the norm. Based on this observation, various degrees of mitral disease are distinguished. By the way, deflection of the front flap is much more common than deflection of the rear flap.
In most cases, children suffer from such cardiac pathology (congenital anomaly). The connective tissue does not have time to fully form, and the valves are initially susceptible to deformation. Often the chords also change. After which they are unable to maintain healthy valve tone.
Attention! It has been established that predominantly women suffer from the disease in question. In view of this, the fetus of the weaker sex while still in the womb requires a more thorough examination and diagnosis.
Provoking factors for the development of the disease
 Doctors say that congenital (primary) prolapse often occurs, which is inherited and depends on the individual characteristics of the human body. However, it can also appear against the background of a certain disease (secondary). The following are distinguished: possible reasons development of pathology:
Doctors say that congenital (primary) prolapse often occurs, which is inherited and depends on the individual characteristics of the human body. However, it can also appear against the background of a certain disease (secondary). The following are distinguished: possible reasons development of pathology:

Attention! Secondary prolapse can occur at any age, regardless of a person’s gender.
Without appropriate treatment, the acquired type of the disease in question quickly develops into a complex form.
Symptoms of the disease
Pathology of the mitral valve itself often occurs without any symptoms. In some cases, the disease enters the second stage of its development without a single sign of the presence of an abnormal process.
Only aching or acute pain on the left side of the chest can cause suspicion. Moreover, this pain syndrome is in no way associated with ischemic disease.
Discomfort does not leave the patient for several minutes or even days. The intensity of pain increases due to stress, nervous tension, excitement. Physical activity does not affect the strength of the pain syndrome. Additional signs of the disease are:

If the above symptoms are detected, the patient should consult a doctor as soon as possible.
Accepted classification
 The degree of progression of the disease at this moment can only be determined by conducting an echocardiographic study.
The degree of progression of the disease at this moment can only be determined by conducting an echocardiographic study.
Depending on the intensity of blood entering the left ventricle, the following stages of pathology are distinguished:

The advanced stage of the disease in question requires surgical intervention.
Diagnostic methods for studying pathology
Detection of the disease in question begins with listening to the heart with a stethoscope. Afterwards, if necessary, they resort to other diagnostic methods, including the following:
- Ultrasound examination of the heart (echocardiography) is one of the most effective ways establishing the degree of pathology, which makes it possible to detect malfunctions in various cardiac structures;
- abnormal heartbeat, as one of the signs of prolapse, will be shown by electrocardiography;
- Using Holter electrocardiography, they monitor not only the rhythm of heart contraction, but also control the treatment of arrhythmia.
 No less effective in recognizing this heart disease are radiography and phonocardiography. In this way, you can detect deformation of a characteristic organ and listen to heart murmurs.
No less effective in recognizing this heart disease are radiography and phonocardiography. In this way, you can detect deformation of a characteristic organ and listen to heart murmurs.
Doppler diagnostics allows you to determine the speed of blood movement.
Further therapy is prescribed strictly after all the results of the examination and tests.
Treatment regimen
Treatment of anterior mitral valve prolapse different ways. The course of therapy depends on the type and degree of development of the anomaly. For congenital pathology, no treatment is carried out at all. After all, medications do not affect the patient’s condition in any way. If the symptoms are pronounced, then therapy is selected taking into account individual characteristics and the severity of the disease.
The standard treatment regimen is as follows:

Improves the general condition of the patient by taking various vitamin complexes. TO surgical intervention resort only as a last resort. During the operation, the damaged valve is replaced.
Complications due to the disease
 It is worth noting that treatment of the disease in question usually has a favorable prognosis. Severe complications, the consequences of this disease develop very rarely.
It is worth noting that treatment of the disease in question usually has a favorable prognosis. Severe complications, the consequences of this disease develop very rarely.
Sometimes arrhythmia or endocarditis of an infectious nature appears. Experts often diagnose the development of thromboembolism as a consequence of the progression of prolapse.
The clinical picture is complemented by symptoms:
- yellowish skin tone;
- fatigue, weakness;
- low pressure;
- joint pain.
 However, the emergence various complications can be minimized if you go to the hospital in time and begin adequate treatment.
However, the emergence various complications can be minimized if you go to the hospital in time and begin adequate treatment.
Prolapse of the mitral valve, namely the anterior leaflet of the mitral valve - quite dangerous disease. It should be treated by a qualified specialist.
Self-prescription of medications is unacceptable. If you adhere to all the instructions of the attending physician, undergo timely examinations and undergo regular therapeutic courses, then the pathology will not be able to affect a person’s quality of life.
Article publication date: November 25, 2016
Article updated date: 12/18/2018
From this article you will learn: characteristics of the pathology of mitral valve prolapse, the causes of its occurrence, classification by severity. Main symptoms, treatment methods, how it can be dangerous, possible restrictions for patients and prognosis for the future.
The mitral or bicuspid valve is the valve that separates the left atrium from the left ventricle. During diastole (relaxation of the ventricles), the valve opens, allowing oxygenated blood from the pulmonary circulation in the left atrium to pass into the left ventricle, from where it then flows through the left atrium. big circle blood circulation
With mitral valve prolapse (abbreviated MVP), flexion or prolapse of the mitral valve leaflets occurs, which, depending on the severity, may either not be accompanied by any symptoms at all and not bother the patient in any way, or lead to quite serious problems, unpleasant manifestations and significant restrictions in terms of professional activities and sports.
With normal structure and function of the mitral valve, it is tightly closed during ventricular systole (contraction) and does not allow blood to return to the atrium. But in the presence of prolapse, the valve leaflets, under blood pressure, bend towards the left atrium and partially open, allowing blood to flow back into the atrium - this process is called regurgitation. The more pronounced the blood regurgitation, the more pronounced the clinical manifestations of MVP.
The prevalence of this pathology among the population is relatively low - it is found in approximately 2.5–3% of people. However, in recent years, due to the introduction of cardiac ultrasound into routine examinations of adolescents and children, mitral valve prolapse is detected much more often, and specifically in patients young and children.
Diagnosis and treatment of prolapse is carried out by cardiologists. They also determine possible restrictions for patients, including with regard to study, work, military service, and physical activity.
Causes
The exact causes of prolapse are unclear. It is believed that the main role is played by the structural features of connective tissue - the so-called connective tissue dysplasia. With connective tissue dysplasia, numerous and varied disorders of the structure and function of those organs that include connective tissue are noted - heart valves, organs of vision, joints, cartilage, etc. Thus, along with prolapse, many patients are found to have myopia and increased mobility (flexibility) of joints, scoliosis and postural disorders.
The following diseases can also lead to mitral valve pathology:
- previous infectious and toxic endocarditis,
- tonsillitis and scarlet fever,
- cardiac ischemia,
- metabolic disorders.
Classification
Mitral valve prolapse is classified according to the degree of deflection of the leaflets:
The degree of prolapse is not always directly related to the severity of the disease. The presence and severity of regurgitation is considered more indicative: the stronger it is, the more serious prognosis, and the more anxiety the pathology causes to patients.
 Types of mitral valve prolapse with regurgitation
Types of mitral valve prolapse with regurgitation Symptoms
Mitral valve prolapse has no specific symptoms. Deflection of the 1st degree in the absence of regurgitation in general most often occurs completely asymptomatically - it is discovered accidentally during medical examination and ultrasound of the heart.
With 2 and 3 degrees of prolapse and the presence of regurgitation, patients can present a variety of complaints, which, however, are more often associated not with prolapse itself, but with background or concomitant pathology (vegetative-vascular dystonia, neuroses, etc.). Most often, patients are concerned about the following symptoms:
- stabbing in nature, which may be associated with physical activity or nervous stress.
- Attacks of tachycardia (palpitations), accompanied by dizziness, weakness, nausea.
- Feeling of heart failure.
- Increased fatigue, the appearance of tiredness and weakness even after minor physical or mental stress.
- Tendency to fainting and pre-fainting states (severe weakness, dizziness) - in stuffy rooms, against a background of emotional stress.
- Feeling of lack of air, pain in the chest when breathing.
- Insomnia, nightmares, waking up with palpitations and heart pain.

Diagnostics
If there are complaints and symptoms of the heart, a cardiologist should prescribe examination and treatment. Because the specific signs prolapse does not exist, after questioning and examining the patient, the doctor can only assume a diagnosis, and to confirm it, it is necessary to conduct a study visualizing the structure and function of the heart - Doppler echocardiography (Echo CG) or ultrasound of the heart.
 Echocardiography can diagnose mitral valve prolapse
Echocardiography can diagnose mitral valve prolapse According to ultrasound data, it is determined that there is mitral valve prolapse, its degree, presence or absence and severity of regurgitation are determined. As a rule, other studies are not needed to clarify the diagnosis, but they may be needed to determine professional or sports suitability.
As additional examination methods, various tests are carried out (test on an exercise bike with an ECG and Echo CG before and after exercise, squat tests, measuring blood pressure in a lying position and immediately after taking a vertical position, etc.). You may also need blood tests (general and biochemical), consultations with related specialists (neurologist, rheumatologist, psychiatrist, cardiac surgeon).
 Exercise bike test with ECG
Exercise bike test with ECG Treatment
In mild forms of the disease, when mitral valve prolapse is mild and regurgitation is absent or minimal, treatment is usually not prescribed. However, treatment may be necessary for those patients who complain of heart pain, fainting and dizziness.
Since such complaints moderate changes The structures and functions of the valve are most often caused not by heart pathology itself, but by neurasthenia, neuroses and other neurological problems, and treatment, accordingly, is prescribed by neurologists (in close cooperation with cardiologists).
- Compliance with the regime - avoid stress, physical and mental overload. It is highly advisable to consult a psychotherapist or psychologist and undergo training in methods of self-control (over emotions, behavior), and relaxation. Required correct mode work (during the day, with normal working hours and a full lunch break). A mandatory component of treatment is a complete night sleep. For sleep disorders, mild sleeping pills are indicated.
- Carrying out activities with a general strengthening effect - hardening, walking in the fresh air, swimming in the pool.
- Drug therapy - sedative (calming) drugs - such as motherwort, valerian, novopassit. Potent tranquilizers are used extremely rarely. Also included are drugs that normalize metabolism (metabolism) in the myocardium - kudesan, elkar, etc.
 Lifestyle recommendations for patients with mild form mitral valve prolapse
Lifestyle recommendations for patients with mild form mitral valve prolapse For grade 2–3 prolapse in combination with regurgitation, when patients are often diagnosed with increased blood pressure and arrhythmias, it is additionally recommended to take antihypertensive and antiarrhythmic drugs. To prevent the development of infective endocarditis in prolapses with regurgitation of degree 2 or more, antibacterial therapy is recommended.
In especially severe cases that do not respond well to conservative treatment, cardiac surgical correction may be recommended. The main indications for surgical intervention are the development of chronic mitral regurgitation and the risk of developing (or already developing) heart defects.
Patient monitoring
Patients who have been diagnosed with mitral valve prolapse, regardless of severity and the presence or absence of regurgitation, should be registered with a cardiologist and undergo regular examinations. It is recommended to perform it at least once a year to assess the dynamics; conducting an ECG 2 times a year – for early detection arrhythmias.
 Patients with mitral valve prolapse are recommended to undergo electrocardiography 2 times a year
Patients with mitral valve prolapse are recommended to undergo electrocardiography 2 times a year The cardiologist determines the patient’s capabilities in terms of professional activities, sports, and suitability for military service. Prolapse of the 1st degree without regurgitation does not impose serious restrictions, only severe ones can be contraindicated physical exercise and training in some higher education institutions educational institutions military orientation ( flight schools and etc.). The question of the possibility of playing sports is decided individually (depending on the type of sport and the presence of complaints).
With prolapses with regurgitation, especially pronounced, the restrictions are much more serious. Professional sports are generally prohibited. Military service is contraindicated; there are contraindications for a number of professions.
Complications
Severe mitral valve prolapse, especially in combination with regurgitation, can lead to the development of such serious complications as:

Forecast
In the vast majority of cases, mitral valve prolapse occurs without complications, causing virtually no discomfort to patients.
The prognosis for grades 1–2 with minimal or no regurgitation is favorable, there are practically no restrictions, and they only relate to significant physical activity.
With prolapse of the 3rd degree or in the presence of severe regurgitation, the prognosis is much more serious, and the course of the pathology is unstable and unpredictable, it is dangerous for its complications, therefore, to improve the patient’s quality of life and reduce risks, cardiac surgical correction of the anomaly may be recommended.
